
Carboxyhemoglobin and methemoglobin levels as prognostic markers in acute pulmonary embolism
a b s t r a c t
Objectives: Carboxyhemoglobin (COHb) and methemoglobin (MetHb) levels have been associated with a poor outcome in patients with various pathological conditions including cardiovascular diseases. Our aim was to retrospectively assess the prognostic value of arterial COHb and MetHb in patients with acute pulmonary embolism (PE).
Methods: We conducted a retrospective study of 156 patients admitted in a pulmonary clinic due to acute PE. Measured variables during emergency department evaluation that were retrospectively analyzed included the ratio of the partial pressure of oxygen in arterial blood to the fraction of oxygen in inspired gas, Acute Physiology and Chronic Health Evaluation II score, risk stratification indices, and arterial blood gases. The association be- tween arterial COHb and MetHb levels and disease severity or mortality was evaluated using bivariate tests and logistic regression analysis.
Results: Arterial COHb and MetHb levels correlated with Acute Physiology and Chronic Health Evaluation II and pulmonary severity index scores. Furthermore, arterial COHb and MetHb levels were associated with troponin T and N-terminal pro-B-type natriuretic peptide levels. In univariate logistic regression analysis, COHb and MetHb levels were both significantly associated with an increased risk of death. However, in multivariate analy- sis, only COHb remained significant as an independent predictor of in-hospital mortality.
Conclusion: Our preliminary data suggest that arterial COHb and MetHb levels reflect the severity of acute PE, whereas COHb levels are independent predictors of in hospital death in patients in this clinical setting. These findings require further prospective validation.
(C) 2015
Introduction
Carboxyhemoglobin (COHb) and methemoglobin (MetHb) are vari- ants of normal hemoglobin, which is contained in red blood cells and is responsible for oxygen’s transportation from lungs to tissue cells. Both molecules are formed from hemoglobin throughout different processes. Carboxyhemoglobin is formed when hemoglobin binds naturally occur- ring and exogenous inhaled carbon monoxide (CO). Endogenous CO is synthesized mainly by heme oxygenase, which catalyses heme catabo- lism to CO, iron, and biliverdin. Carbon monoxide has been reported to take part in a variety of pathological functions such as vasodilation, angiogenesis, vascular remodeling, and inflammatory response [1,2].
? Conflict of interest: The authors declare that they have no conflict of interest or finan- cial ties to disclose.
* Corresponding author at: Pulmonary Department, Evangelismos General Hospital of Athens, Ypsilanti 45-47, 10676 Athens, Greece. Tel.: +30 213 2041631; fax: +30 210
7232370.
E-mail addresses: [email protected] (S. Kakavas), [email protected] (A. Papanikolaou), [email protected] (E. Ballis), [email protected] (N. Tatsis), [email protected] (C. Goga), [email protected] (G. Tatsis).
The reported blood COHb saturation is approximately 1% in nonsmokers and about 5.5% in smokers with a smoking history of almost 20 ciga- rettes/d [3,4]. A number of studies have described significantly altered COHb levels in several pathological conditions including lower respira- tory tract infections, critical disease, and cardiopulmonary arrest [5-8]. More importantly, in these studies, COHb levels have been associated with the severity of the clinical course and/or the outcome of the pa- tients. Interestingly, both low minimum and high maximum levels of COHb were associated with increased mortality in critically ill patients after a cardiothoracic surgery [6]. An estimated elevated level of COHb appeared to be associated with a more severe course in patients with an acute ischemic disease, too [9].
On the other hand, MetHb formation is the result of an oxidative pro- cess during which 1 or more of the 4 iron atoms in the hemoglobin mol- ecule convert to ferric state and therefore are incapable of binding oxygen. Endogenous MetHb is produced when naturally produced Nitric oxide interacts with hemoglobin. Methemoglobin may also be tem- porally formed during unloading of oxygen from deoxyhemoglobin in tis- sues. Large amounts of NO may be produced in various forms of critical illness such as sepsis or septic shock. As a result, increased levels of NO may be released in the circulation and enhance the formation of MetHb. In fact, increased MetHb levels have been demonstrated in patients
http://dx.doi.org/10.1016/j.ajem.2015.01.046
0735-6757/(C) 2015
with sepsis. Furthermore, in these patients, increased MethHb levels have been reported to correlate with a more severe course of sepsis [10].
Acute pulmonary embolism (PE) represents a potentially fatal med- ical condition, especially when associated with hemodynamic instabili- ty or signs of right ventricular dysfunction [11,12]. Current guidelines prognostically stratify patients with PE into 3 classes accord- ing to early mortality risk: high-risk PE with a short-term mortality greater than 15%, including hemodynamically unstable patients; inter- mediate risk PE, depending on the identification of either RV dysfunc- tion or blood markers of myocardial injury; and low-risk PE. Early mortality risk refers to in-hospital or 30-day mortality [13,14]. Never- theless, prognostication in PE remains an unsettled issue, and there is an ongoing need for the identification of markers that can be incorpo- rated into the clinical practice and improve the Predictive ability of early stratification in patients with PE. Prognostic assessment is also useful for the selection of the Optimal treatment for every risk class of patients. To date, there are no data on arterial COHb and MetHb levels in patients with acute PE, nor has the predictive ability of these param- eters been evaluated in patients in this clinical setting. We therefore un- dertook a retrospective observational study of a small cohort of patients with acute PE. The aim of this study was to test the ability of arterial COHb and MetHb levels to predict in-hospital mortality in this group of patients.
Methods
Subjects
The present study was approved by the institutional ethics commit- tee. The nature of the study was observational and retrospective. There- fore, the need for informed, written consent was waived by the same committee. The study included all eligible patients diagnosed as having acute PE who were consecutively admitted to the pulmonary clinic of a tertiary general hospital from January 2012 through July 2014. We ana- lyzed 192 consecutive patients hospitalized in our department with PE, confirmed with computed tomographic (CT) pulmonary angiography. Demographic characteristics and clinical information including smoking status are collected at least twice in our hospital. Initially, the personal history and clinical details concerning each patient are recorded in the emergency department (ED). After admission, the patient’s personal history is reverified later in the clinic and it is finally stored electronical- ly. We examined both forms of medical records (handwritten and elec- tronic). In the event of unrecoverable or unrecorded data or if any discrepancy appeared in either one of the sources, the respective case was rejected. Furthermore, the exclusion criteria included positive smoking status at the time of admission and absence of blood gas anal- ysis on arrival. Twenty-two patients were excluded due to positive smoking status at the time of the admission, whereas 4 patients were excluded because they did not undergo blood gas analysis on arrival. Another 10 patients were excluded because various data could not be retrieved. The final study sample consisted of 156 patients, whose char- acteristics are reported in Table 1.
Study design
From medical records, we obtained demographic characteristics, clinical information, complete blood counts and biochemical values, treatment received on admission or during the in-hospital period, the outcome, and length of hospitalization. A series of variables determined at the time of the patients arrival were analyzed, including the follow- ing: sex, age, pH, PO2, PCO2, HCO-, COHb, MetHb, mean arterial pressure, markers of RV dysfunction and/or Myocardial necrosis, initial risk strat- ification, and therapeutic modality. Acute Physiology and Chronic Health Evaluation II score (ranging from 0 to 71) and Pulmonary Embolism Severity Index (PESI) at the time of arrival was
3
Table 1
Characteristics of study population
Variable Median (range) or no. (%)
|
Age (y) |
76 (20-95) |
|
Sex (male) |
77 (49.4) |
|
16 (3-30) |
|
|
PESI |
117.5 (40-246) |
|
PaO2/FIO2 |
278.5 (95-484) |
|
Hospital days |
8 (4-23) |
|
PaCO2 (mm Hg) |
35.3 (23.2-63) |
|
HCO3 (mmol/L) |
23.25 (13.5-28.7) |
|
COHb (%) |
1.20 (0.3-2.6) |
|
MetHb (%) |
0.5 (0.2-1.2) |
|
Hemoglobin (mg/dL) |
12.55 (9.00-15.4) |
|
Leukocyte count (103/mm3) |
10170 (3420-20670) |
|
Creatinine (mg/dL) |
1.08 (0.56-2.80) |
|
D-Dimers (mg/L) |
2.5 (0.44-10.39) |
cTnT (pg/mL) 53.5 (3-206)
NT-proBNP (pg/mL) 351 (12-6348)
Echo or ECG indices of RV dysfunction 69 (44.2)
PaCO2, partial pressure of carbon monoxide, arterial; Echo, echocardiography; ECG, electrocardiogram.
calculated based on the appropriate baseline clinical, demographic, and serologic characteristics of each patient using the values retrieved from the computerized medical records system.
According to the standard Diagnostic protocol of our hospital, clinical history and physical examination were performed in all patients upon presentation to the ED and after admission to our clinic. Demographic and clinical characteristics, including age, heart rate, respiratory rate, systolic blood pressure, and diastolic blood pressure of all patients were obtained. Arterial blood gases were measured shortly after pre- sentation to the ED, and the ratio of the partial pressure of oxygen in ar- terial blood to the fraction of oxygen in inspired gas (PaO2/FIO2) was calculated. In addition, a 20-mL blood sample was taken and an intrave- nous line was established. In patients with compatible clinical history and/or suggestive clinical findings, PE was confirmed based on CT pul- monary angiography.
Patients diagnosed as having acute PE were classified, based on early mortality risk, in groups of high, intermediate-high, intermediate-low, and low risk. This initial risk stratification was based on the presence of the following risk markers [13,14]:
Hemodynamic instability was diagnosed in patients with the pres- ence of at least one of the following criteria: (1) sustained hypotension (systolic blood pressure b 90 mm Hg or a pressure decrease of >=40 mm Hg for N 15 minutes at arriving in the ED or requiring vasoactive sup- port) that could not be attributed to an alternative diagnosis (arrhyth- mia, acute left ventricular dysfunction, acute coronary syndrome, hypovolemia, or sepsis), (2) cardiac arrest (pulselessness), and (3) per- sistent Symptomatic bradycardia (heart rate b 40 beats/min with signs or symptoms of shock). Patients with hemodynamic instability were considered affected by high-risk PE and therefore as candidates for thrombolytic therapy.
A PESI score greater that 85 points was considered as indicative of in- termediate risk in Hemodynamically stable patients. Patients character- ized by intermediate-risk status and at the same time imaging and biochemical findings compatible with RV dysfunction and/or myocardi- al necrosis were classified as intermediate-high-risk patients. Con- versely, a PESI score higher than 85 points without further findings classified the patient in the intermediate-low-risk group. Elevated levels of Cardiac troponin T (cTnT; N 100 pg/mL) were considered as in- dicative of myocardial necrosis. right ventricular dysfunction was con- firmed by the presence of at least one of the following: (1) RV systolic dysfunction on echo; (2) RV dilation (Apical 4-chamber RV diameter di- vided by LV diameter N 0.9) on CT; (3) RV dilatation, hypokinesis, or pressure overload on echo; or (4) elevation of N-terminal pro-B-type natriuretic peptide (NT-proBNP; N 500 pg/mL). Echocardiography was
performed by a skilled cardiologist using standard views with a GE Logiq e Portable Ultrasound device (General Electric Company, Wauwatosa, WI) using a 2.4-MHz multiplane transducer.
Finally, hemodynamically stable patients with acute PE and a PESI score less than 85, with no RV dysfunction or myocardial necrosis were considered as low risk.
All patients received supportive therapy at the time of admission, and they were treated according to guidelines after the confirmation of PE di- agnosis. Briefly, oxygen was supplied to achieve an arterial oxygen satura- tion of 92% or greater. Hemodynamically stable patients received standard anticoagulation therapy with intravenous unfractionated heparin or subcutaneous low-molecular-weight heparin. Thrombo- lytic therapy was conferred for patients with hemodynamic instabil- ity and no high risk of bleeding. Collectively, 35 patients received thrombolysis (2-hour infusion of 100 mg recombinant tissue plas- minogen activator). All patients with diagnosed acute PE were ad- mitted to the pulmonary clinic.
Measurements
Levels of COHb and MetHb were determined immediately upon ED admission using a heparinized blood sample that was collected by puncture from a peripheral artery. Determination was performed using a Blood gas analyzer (ABL 700 Radiometer, Copenhagen, Denmark) that automatically measures the pH, PO2, PCO2, HCO-, base excess, COHb, and MetHb. The analyzer runs a zero calibration of the optical system against a colorless calibration fluid at least every 4 hours to guarantee accuracy.
3
Complete blood counts and biochemical values retrospectively eval- uated were measured from blood samples obtained by peripheral vein puncture upon admission to the ED. Serum Creatinine levels were mea- sured on a Roche/Hitachi Modular System P (Roche Diagnostics GmbH, Mannheim, Germany) by enzymatic assay. Serum cTnT levels were measured using the electrochemiluminescence immunoassay on a Roche modular system E170 (Roche Diagnostics GmbH). Serum NT- proBNP was determined using an electrochemiluminescence immuno- assay method (NT-proBNP; Roche) with a Roche modular E170 immu- noassay analyzer (Roche Diagnostics GmbH). Other biochemical measurements and electrolyte levels were determined by standard lab- oratory methods.
For the measurement of the aforementioned parameters in all el- igible subjects, blood samples were obtained shortly after the admis- sion of patients to the ED. Therefore, in all the cases, blood was obtained before the administration of anticoagulants or thromboly- sis. The outcome variables recorded included mortality and length of hospital stay.
Statistical analysis
Continuous variables are reported as medians and ranges, and cate- gorical variables are expressed as percentages. Continuous variables were compared by the unpaired-samples Mann-Whitney test. Associa- tion between variables was assessed by spearman correlation coeffi- cient. Univariate logistic regression analyses were performed to examine the association between mortality and each of the predictors separately in order to identify factors significantly associated with an in- creased risk of death; for each variable, the odds ratio (OR), and 95% confidence interval (CI) are given. All variables with P b .1 variables were then tested in a multivariable logistic regression analysis model aiming to the identification of independent predictors of in- hospital mortality.
A 2-sided P value less than .05 was considered statistically signifi- cant. All analyses were performed using SPSS version 13.0 software (SPSS, Inc, Chicago, IL).
Results
A total of 156 patients (77 men and 79 women) were enrolled into the present study. Patients’ baseline clinical and laboratory data are re- ported in Table 1. The mean COHb and MetHb levels in all patients were 1.41% (0.3%-2.6%) and 0.57% (0.2%-1.2%), respectively. Both COHb and MetHb levels were significantly correlated with APACHE score (Fig. 1A and B). However, only MetHb levels showed a significant inverse corre- lation (? = -0.335, P b .001) with the severity of pulmonary gas ex- change impairment, as reflected by the PaO2/FIO2 ratio. In this study sample, the length of in hospital stay correlated positively with MetHb levels (? = 0.456, P b .001) and negatively with COHb (? = - 0.279, P b .05). Furthermore, the length of in hospital stay was negatively corre- lated with PaO2/FIO2 ratio (? = -0.368, P b .001) and positively correlat- ed with APACHE score (? = 0.253, P b .01) and Nt-proBNP levels (? = 0.255, P b .01).
Statistical analysis revealed significantly lower COHb levels in pa- tients with increased risk of early mortality (high- and intermediate high-risk groups; P b .001; median COHb, 1.1%; range, 0.3%-2.6%; n =
69) than in patients with low risk of early mortality (low- or intermedi- ate low-risk groups; median COHb, 1.4%; range, 1%-2.5%; n = 87). On the other hand, significantly higher MetHb levels characterized patients with increased risk of early mortality (P b .001; median MetHb, 0.8%; range, 0.2%-1.1%; n = 30) in comparison with low- and intermediate low-risk patients (median MetHb, 0.4%; range 0.2%-1.1%; n = 46). In ac- cordance with these findings, a significant inverse correlation was found between COHb levels and cTnT (? = - 0.265, P b .01) or NT- proBNP levels (? = -0.344, P b .01). Similarly, MetHb levels correlated significantly not only with cTnT levels (? = 0.329, P b .01) but also with NT-ProBNP levels (? = 0.443, P b .001). The correlation analysis of COHb and MetHb levels with the parameters used in the early strat- ification of patients with PE is shown in Table 2.
In this cohort, 16 (10.25 %) of the 156 patients died during their stay in the pulmonary clinic. No significant difference was observed between these patients and those who survived in terms of age, sex, leukocyte
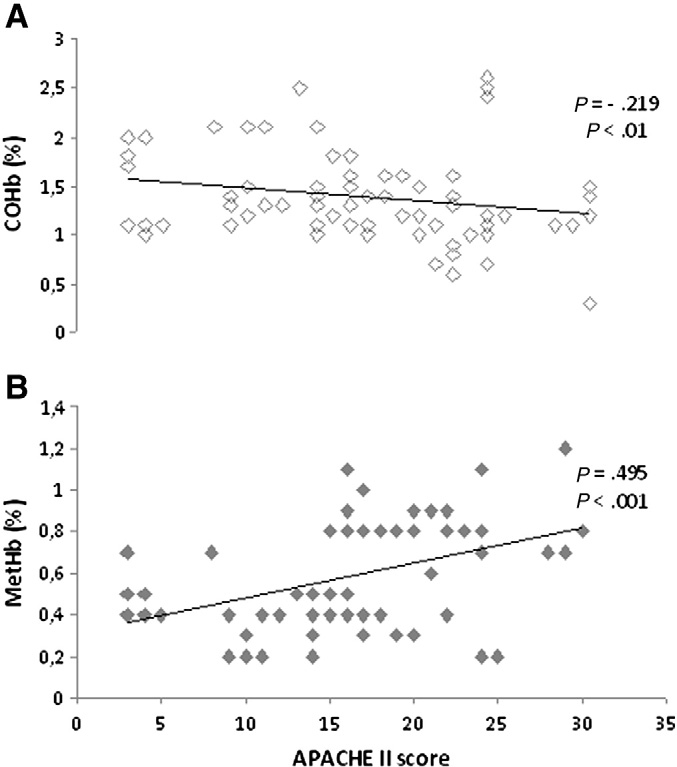
Fig. 1. A, Relationship between plasma levels of COHb and APACHE II score. B, Relationship between plasma levels of MetHb and APACHE II score. Data were obtained in 156 patients with acute PE upon admission to the ED.
Correlation analysis of COHb and MetHb levels with the PESI and serum markers of myo- cardial injury and RV function
Table 3
Univariate logistic regression analysis of predictive factors associated with survival in pa- tients with acute PE
|
Variables |
cTnT |
NT-proBNP |
PESI score |
Variables |
P |
OR |
95% CI |
|
|
COHb |
? = -0.265, P b .01 |
? = -0.344, P b .001 |
? = -0.232, P b .01 |
COHb |
.028 |
4.861 |
1.188-19.887 |
|
|
MetHb |
? = 0.329, P b .001 |
? = 0.443, P b .001 |
? = 0.601, P b .001 |
MetHb |
.001 |
0.024 |
0.002-0.23 |
|
|
PaO2/FIO2 ratio |
.001 |
1.011 |
1.004-1.018 |
|||||
|
APACHE II score |
.004 |
0.841 |
0.769-0.922 |
count, hemoglobin levels, or creatinine. However, as shown in Fig. 2A
|
cTnT |
.044 |
0.992 |
0.984-1.000 |
|
D-Dimers |
.727 |
1.041 |
0.831-1.303 |
|
and B, patients who died were characterized by significantly lower |
Age |
.198 |
0.968 |
0.922-1.017 |
|
COHb levels (P b .05; median COHb, 1.15%; range, 0.6%-1.5%) and higher |
Creatinine |
.569 |
0.777 |
0.326-1.851 |
|
MetHb levels (P b .001; median MetHb, 0.8%; range, 0.4%-0.9%) in com- parison with patients who survived (median COHb levels, 1.25% [range, |
NT-proBNP WBC |
.338 .120 |
1.000 1.000 |
1.000-1.001 1.000-1.000 |
0.3%-2.6%], and median MetHb, 0.5% [range, 0.2%-1.2%]). Moreover, APACHE II score was significantly higher (P b .01) in patients who died (median APACHE II score, 22.5; range, 16-30) than that in those who survived (median APACHE II score, 14.5; range, 3-30). Finally, cTnT levels were significantly higher (P b .01) in patients who died (me- dian cTnT, 82.5 pg/mL; range, 53-206 pg/mL) than in those who sur- vived (median cTnT, 37.395 pg/mL; range, 3-200 pg/mL).
In univariate logistic regression analysis, both COHb and MetHb levels showed a significant association with an increased risk of death. The results of univarite analysis are presented in Table 3. Multivariate logistic regression analysis, including variables with P b .1, was per- formed to identify factors with independent predictive value for in hos- pital mortality, controlling for possible confounders. Only COHb levels and PaO2/FIO2 ratio were independently related to increased risk of death. The results of multivariate analysis are shown in Table 4.
Discussion
The present retrospective study evaluated and tested the prognostic value of COHb and MetHb levels measured at admission in patients with PE. The importance of immediate clinical assessment in conjunction with the identification of markers leading to more effective risk stratifi- cation of patients with PE is widely accepted. Ideally, these Prognostic markers should promptly and easily accessible in daily clinical practice. Carboxyhemoglobin and MetHb measurement is an easily achieved technique using a blood gas analyzer in the ED. To our knowledge, the present study is the first investigation of COHb and MetHb levels in pa- tients with acute PE. In our study, these parameters correlated with the
WBC, white blood cell count.
disease severity, the risk status, and the pulmonary Gas exchange im- pairment, as reflected by APACHE II score, the levels of cTnT and NT- proBNP and PaO2/FIO2 ratio, respectively.
The present results seem to be in accordance with previous studies
relating COHb levels with severity and prognosis in a variety of critical diseases [6,7]. These clinical settings include not only inflammatory con- ditions such as sepsis, community-acquired pneumonia, and systemic inflammatory response syndrome but also cardiovascular disorders such as acute ischemic disease or postresuscitation care after cardiore- spiratory arrest [5,8-10,15]. In patients after cardiothoracic surgery, in- creased intensive care mortality was associated with both low minimum and high maximum levels [6]. In our study, lower initial COHb levels were associated with a higher APACHE II score and a lower PaO2/FIO2 ratio. On the other hand, increased initial MetHb levels were accompanied by a greater disease severity and a more prominent gas exchange impairment upon admission. Similarly, elevated MetHb levels have been reported in patients with sepsis or septic shock, possi- bly due to the enhanced production of NO that accompanies sepsis. Fur- thermore, increased MetHb levels demarcated the onset of sepsis or septic shock and were associated with the Severity of disease defined by Sequential Organ Failure Assessment score [10].
According to our results, COHb and MetHb are characterized by a significant-inverse or positive respectively-correlation with cTnT and NT-proBNP levels. Levels of NT-proBNP and troponin have been shown to be independent predictors of short-term mortality in patients with acute PE [14]. Furthermore, we found that patients with hemodynamic
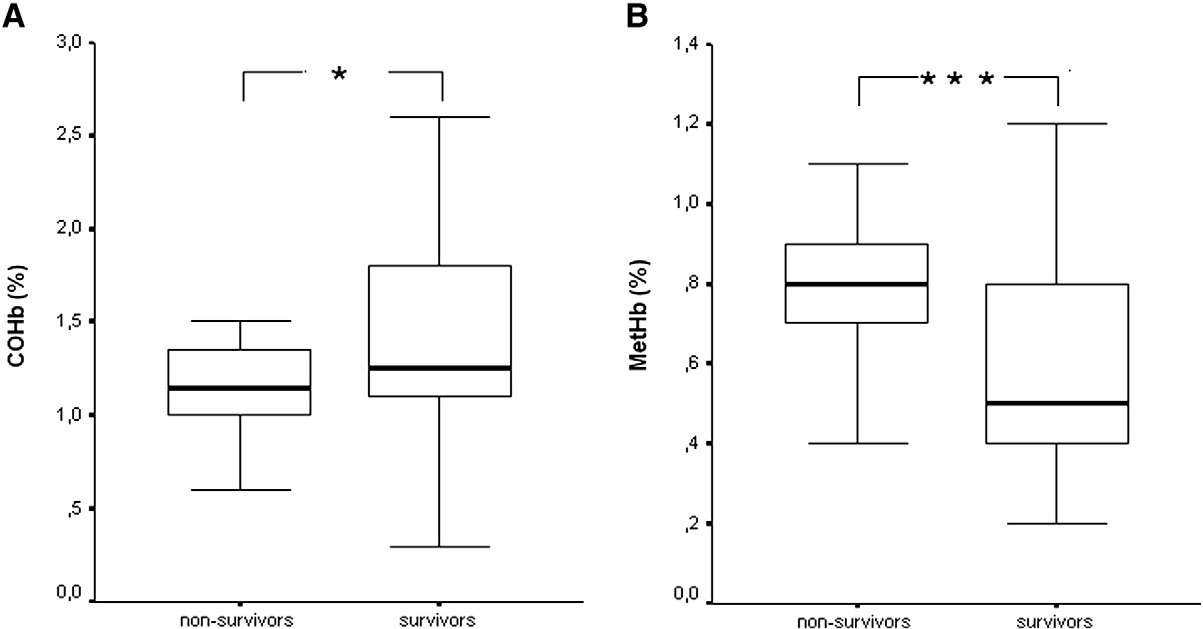
Fig. 2. Comparison of COHb (A) and MetHb (B) levels between survivors (n = 140) and nonsurvivors (n = 16) from acute PE. *P b .05;** P b .01.
Table 4 Multivariate logistic regression analysis of risk factors associated with mortality in patients with acute PE
|
Variables |
P |
OR |
95% CI |
|
COHb |
.047 |
3.688 |
1.017-13.377 |
|
MetHb |
.169 |
0.143 |
0.092-0.265 |
|
APACHE II score |
.09 |
0.902 |
0.801-1.016 |
|
cTnT |
.69 |
0.997 |
0.955-1.010 |
|
PaO2/FIO2 |
.023 |
1.011 |
1.002-1.021 |
instability (high risk of early death) or signs of RV dysfunction or myo- cardial necrosis (intermediate risk of early death) were characterized by lower levels of COHb and higher levels of MetHb in comparison with low-risk patients [14]. This finding may imply that PE hemody- namic compromise may be accompanied by an overproduction of NO or by a diminished production of CO. Such an overproduction of NO has been described in the case of sepsis [10]. Moreover, exogenous CO administered at low concentrations exhibits antioxidative, anti- inflammatory, antiproliferative, and Antiapoptotic effects [16,17]. Like- wise experimentally, CO can ameliorate Ischemia-reperfusion injury in various organs including the heart, lung, kidney, and liver [18-25]. In any case, our results show that COHb and MetHb levels may serve as an additional marker of Hemodynamic compromise, poor RV function, or myocardial injury in patients with acute PE.
Patients who died in our study were characterized by significantly lower COHb levels and higher MetHb levels compared with patients who survived. This finding further amplifies our initial hypothesis that COHb and MetHb levels may be used as additional or a surrogate prog- nostic marker of outcome during initial risk stratification in patients with acute PE. Likewise univariate logistic regression analysis revealed a strong association of survival with COHb and MetHb levels. In fact, COHb levels were the stronger independent predictor of in-hospital mortality in univariate logistic regression analysis.
Obviously, the aforementioned results must be interpreted with caution. For example, it is a fact that exhaled CO and, consequently, COHb levels are influenced by the delivery of High-flow oxygen [26,27]. In addition, our results also show that PaO2/FIO2 ratio is indepen- dently related to increased risk of death in patients with acute PE. Therefore, it could be argued that the observed association between COHb levels and risk of death is actually the result of the coexisting ox- ygen therapy. However, COHb levels remain an independent predictor of survival even after multivariate analysis, controlling for possible con- founders. Furthermore, although a separate analysis excluding patients already on oxygen was not possible, our institution’s emergency proto- col strongly suggests arterial blood analysis very shortly after the patient’s initial presentation. Therefore, samples used for blood gases analysis were drawn before (or very shortly after) initiation of oxygen therapy. Thus, the resultant effect of oxygen therapy on COHb levels may be considered as minimal, although it should be taken into account and ideally such an effect should be quantified. According to our results, MetHb levels correlate with various parameters indicative of the disease severity or RV compromise. On the other hand, the MetHb formation is characterized by a significant interindividual variability metabolically originated in the face of various endogenous or exogenous triggers [28,29]. Certainly, this observed interindividual variability of MetHb concentration may limit the clinical relevance of the results in our study. Even so, from a pathophysiological point of view, our findings warrant further consideration and could serve as the initiative trigger for further evaluation by means of future in vitro experiments or larger prospective studies.
Limitations
Our study has its limitations. The main limitation of this study is its retrospective observational design. Consequently, the data of a few pa- tients could not be retrieved. However, it was possible to verify the
data included in our study from different sources (medical records hand- written and electronic), and therefore, we consider them to be adequate- ly precise. An additional limitation of our study is driven by the difficulty in achieving a given FIO2 in nonintubated individuals. It is true that the presumed FIO2 may be, in fact, variable to a certain degree in the absence of intubation even if high flow oxygen is provided via a venturi mask sys- tem, Ilta Medical, Thessaloniki, Greece. Thus, the calculation of the re- spective PaO2/FIO2 ratio may be roughly but only approximately achieved. Another limitation is the small number of patients in each subgroup that makes statistical analysis difficult. Thus, our results should be interpreted with caution. In addition, the small size of our study sample hinders any attempt to further clarify the pathophysiological pathways leading to the observed alterations. In any case, the potential Prognostic ability of COHb and MetHb levels seems compatible with their implica- tion in pathological conditions characterized by a prominent inflammato- ry response or a significant hemodynamic compromise. The preliminary observations of our study require further validation in larger prospective populations in order to clarify the underlying mechanisms and further verify the prognostic ability of COHb and MetHb levels. This would be of particular value because these indices are widely and readily available
in everyday clinical practice.
Conclusion
In this preliminary study, baseline COHb levels were a strong predic- tor of mortality in patients with acute PE. Levels of COHb and MetHb sig- nificantly correlated with the severity as reflected by the APACHE II score and with impairment of oxygenation as reflected by the PaO2/ FIO2 ratio. Furthermore, COHb and MetHb correlated with PESI score and with baseline NT-proBNP and cTnT levels that are used for the early stratification of patients as markers, indicating the risk of early death from PE.
References
- Li L, Hsu A, Moore PK. Actions and interactions of nitric oxide, carbon monoxide and hydrogen sulphide in the cardiovascular system and in inflammation-a tale of three gases! Pharmacol Ther 2009;123:386-400.
- Wu L, Wang R. Carbon monoxide: endogenous production, physiological functions, and pharmacological applications. Pharmacol Rev 2005;57:585-630.
- Coburn RF, Forster RE, Kane PB. Considerations of the physiological variables that de- termine the Blood carboxyhemoglobin concentration in man. J Clin Invest 1965;44: 1899-910.
- Hart CL, Smith GD, Hole DJ, Hawthorne VM. Carboxyhaemoglobin concentration, smoking habit, and mortality in 25 years in the Renfrew/Paisley prospective cohort study. Heart 2006;92:321-4.
- Corbacioglu SK, Kilicaslan I, Bildik F, Guleryuz A, Bekgoz B, Ozel A, et al. Endogenous carboxyhemoglobin concentrations in the assessment of severity in patients with community-acquired pneumonia. Am J Emerg Med 2013;31:520-3.
- Melley DD, Finney SJ, Elia A, Lagan AL, Quinlan GJ, Evans TW. Arterial Carboxyhemoglobin level and outcome in critically ill patients. Crit Care Med 2007;35:1882-7.
- Fazekas AS, Wewalka M, Zauner C, Funk GC. Carboxyhemoglobin levels in medical intensive care patients: a retrospective, observational study. Crit Care 2012;16:R6. http://dx.doi.org/10.1186/cc11138.
- Youichi Y. Significance of the carboxyhemoglobin level for out-of-hospital cardiopul- monary arrest. J Emerg Trauma Shock 2012;5(4):338-41.
- Mall T, Grossenbacher M, Perruchoud AP, Ritz R. Influence of moderately elevated levels of carboxyhemoglobin on the course of acute ischemic heart disease. Respira- tion 1985;48:237-44.
- Schuerholz T, Irmer J, Simon TP, Reinhart K, Marx G. methemoglobin level as an in- dicator for disease severity in sepsis. Crit Care 2008;12:448.
- Grifoni S, Olivotto I, Cecchini P, Pieralli F, Camaiti A, Santoro G, et al. Short-term clin- ical outcome of patients with acute pulmonary embolism, normal blood pressure, and echocardiographic right ventricular dysfunction. Circulation 2000;101:2817-22.
- Kucher N, Rossi E, De Rosa M, Goldhaber SZ. prognostic role of echocardiography among patients with acute pulmonary embolism and a systolic arterial pressure of 90 mm Hg or higher. Arch Intern Med 2005;165:1777-81.
- Jaff MR, McMurtry MS, Archer SL, Cushman M, Goldenberg N, Goldhaber SZ, et al. American Heart Association Council on Cardiopulmonary, Critical Care, Periopera- tive and Resuscitation; American Heart Association Council on Peripheral Vascular Disease; American Heart Association Council on Arteriosclerosis, Thrombosis and Vascular Biology. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hyper- tension: a scientific statement from the American Heart Association. Circulation 2011;123:1788-830.
- Konstantinides S, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D, Galie N, et al. Authors/ Task force members. Eur Heart J 2014;35:3033-69 3069a-3069k [pii: ehu283].
- Schmidt JE, Morgan JI, Rodriguez-Galindo C, Webb DL, Liang H, Tamburro RF. Heme oxygenase-1 Messenger RNA expression is induced in peripheral blood mononucle- ar cells of pediatric cancer patients with systemic inflammatory response syndrome. Pediatr Crit Care Med 2004;5:554-60.
- Pae HO, Oh GS, Choi BM, Chae SC, Kim YM, Chung KR, et al. Carbon monoxide pro- duced by heme oxygenase-1 suppresses T cell proliferation via inhibition of IL-2 pro- duction. J Immunol 2004;172:4744-51.
- Otterbein LE. The evolution of carbon monoxide into medicine. Respir Care 2009;54:
Kaizu T, Nakao A, Tsung A, Toyokawa H, Sahai R, Geller DA, et al. Carbon monoxide inhalation ameliorates cold ischemia/reperfusion injury after rat liver transplanta- tion. Surgery 2005;138:229-35.
- Faller S, Hoetzel A. Carbon monoxide in acute lung injury. Curr Pharm Biotechnol 2012;13:777-86.
- Ryter SW, Kim HP, Nakahira K, Zuckerbraun BS, Morse D, Choi AM. Protective func- tions of heme oxygenase-1 and carbon monoxide in the respiratory system. Antioxid Redox Signal 2007;9:2157-73.
- Biermann J, Lagreze WA, Dimitriu C, Giallongo C, Palumbo GA, Raciti G, et al. Precon- ditioning with inhalative carbon monoxide protects rat retinal ganglion cells from ischemia/reperfusion injury. Invest Ophthalmol Vis Sci 2010;51:3784-91.
- Nakao A, Kaczorowski DJ, Wang Y, Cardinal JS, Buchholz BM, Sugimoto R, et al. Ame- lioration of rat cardiac cold ischemia/reperfusion injury with inhaled hydrogen or carbon monoxide, or both. J Heart Lung Transplant 2010;29:544-53.
- Yoshida J, Ozaki KS, Nalesnik MA, Ueki S, Castillo-Rama M, Faleo G, et al. Ex vivo ap- plication of carbon monoxide in UW solution prevents transplant-induced renal is- chemia/reperfusion injury in pigs. Am J Transplant 2010;10:763-72.
- Ikeda A, Ueki S, Nakao A, Tomiyama K, Ross MA, Stolz DB, et al. Liver graft exposure to carbon monoxide during cold storage protects sinusoidal Endothelial cells and ameliorates reperfusion injury in rats. Liver Transpl 2009;15:1458-68.
- Katada K, Bihari A, Mizuguchi S, Yoshida N, Yoshikawa T, Fraser DD, et al. Carbon mon- oxide liberated from CO-releasing molecule (CORM-2) attenuates ischemia/reperfusion (I/R)-induced inflammation in the Small intestine. Inflammation 2010;33:92-100.
- Weaver LK, Howe S, Hopkins R, Chan KJ. Carboxyhemoglobin half-life in carbon monoxide-Poisoned patients treated with 100% oxygen at atmospheric pressure. Chest 2000;117(3):801-8.
- Zegdi R, Caid R, Van De Louw A, Perrin D, Burdin M, Boiteau R, et al. Exhaled carbon monoxide in mechanically ventilated critically ill patients: influence of inspired ox- ygen fraction. Intensive Care Med 2000;26:1228-31.
- Wright RO, Lewander WJ, Woolf AD. Methemoglobinemia: etiology, pharmacology, and clinical management. Ann Emerg Med 1999;34:646-56.
- Weinberger B, Laskin DL, Heck DE, Laskin JD. The toxicology of inhaled nitric oxide. Toxicol Sci 2001;59:5-16.