



Abstract
The clinical course of COVID-19 presents a broad spectrum, being asymptomatic in some individuals while following a severe course and resulting in mortality in others. It is known that such factors as age and chronic diseases can result in a different clinical courses in individuals, however, variable clinical courses among the similar individuals in terms of age and chronic diseases are also seen. Other possible factors affecting the course of the disease that are mostly speculative or under investigation are genetic factors and the origin of transmission or possible subtype of novel coronavirus. Whether the source of transmission is important in the clinical course of the disease is unknown.
A case series composed of seven individuals in a similar age group, with different lines of descent and different genetic structures, but who were infected from the same source is presented here. The similar and different clinical, laboratory and radiological findings of the cases residing in the same nursing home, who presented to the hospital altogether, were evaluated. The aim of the study was to analyze whether the source of transmission is influential in the clinical course of the disease.
Keywords
1. Introduction
According to World Health Organization (WHO) data, the confirmed number of novel Coronavirus Disease (COVID-19) cases as of April 26, 2020 is 2,719,897, with 187,705 mortalities [
1
]. WHO declared a “Public Health Emergency of International Concern” on January 30, 2020 and a global “Pandemic Outbreak” on March 11, 2020 due to the rapid spread of COVID-19, which had become a significant global health problem, affecting millions of people in many countries [2
,3
,4
]. No efficacious drug has yet been found, nor a vaccine developed for the treatment of COVID-19, which has come to affect the entire world over the last 5 months. The treatment and the development of a vaccine for this viral disease will be possible following the determination of the characteristics of the virus, and the changes and damages it inflicts on the human metabolism.Some individuals infected by the SARS-CoV-2, which causes the COVID-19 disease, are asymptomatic or manifest mild symptoms, while severe respiratory distress syndrome or death develops in others [
5
,- Inui S.
- Fujikawa A.
- Jitsu M.
- et al.
Chest CT findings in cases from the cruise ship “diamond princess” with coronavirus disease 2019 (COVID-19).
Cardiothorac Imaging. Mar 17, 2020; 2https://doi.org/10.1148/ryct.2020200110
6
]. Some of the factors that predict the course of the disease are known. For example, advanced age and accompanying comorbidities have been defined as an indicator of a severe course of the disease [- Guan W.
- Ni Z.
- Hu Yu
- Liang W.
- et al.
Clinical characteristics of coronavirus disease 2019 in China.
N Engl J Med. Feb 28, 2020; https://doi.org/10.1056/NEJMoa2002032
6
,- Guan W.
- Ni Z.
- Hu Yu
- Liang W.
- et al.
Clinical characteristics of coronavirus disease 2019 in China.
N Engl J Med. Feb 28, 2020; https://doi.org/10.1056/NEJMoa2002032
7
]. It was also previously reported that SARS-CoV-2 may affect those of the male gender [6
,- Guan W.
- Ni Z.
- Hu Yu
- Liang W.
- et al.
Clinical characteristics of coronavirus disease 2019 in China.
N Engl J Med. Feb 28, 2020; https://doi.org/10.1056/NEJMoa2002032
7
] and with the A blood type more [8
]. That said, the factors predicting the course of the disease are still unclear. Genetic factors of hosts are among the possible factors, although it is reported in some case reports that the course of the disease can differ or be similar in individuals of the same family in familial clusters [Zhao J, Yang Y, Huang H, et al. Relationship between the ABO blood group and the COVID-19 susceptibility. medRxiv 2020.03.11.20031096; doi:https://doi.org/10.1101/2020.03.11.20031096.
9
, - Qian G.
- Yang N.
- Yan Ma A.H.
- et al.
COVID-19 transmission within a family cluster by presymptomatic carriers in China.
Clin Infect Dis. 2020; https://doi.org/10.1093/cid/ciaa316
10
, 11
]. As such, the role of genetics in the COVID-19 disease is still controversial, and new studies are needed on this subject. Another topic of discussion is the source of transmission of the virus. In other words, it is unclear whether the course of the disease will be severe in a patient who contracted the disease from a host with a severe course, or vice versa, whether the disease course will be mild in a patient that has contracted the disease from a host with a mild course. Recently, Forster and colleagues have shown that the virus has more than one subtype [- Li P.
- Fu J.B.
- Li K.F.
- et al.
Transmission of COVID-19 in the terminal stage of incubation period: a familial cluster.
Int J Infect Dis. Mar 16, 2020; ([S1201 9712(20)30146-6])https://doi.org/10.1016/j.ijid.2020.03.027
12
]. Therefore, one of the reasons for the course of the disease to be different in individuals may be the source factor, ie subtypes of the novel coronovirus.- Forster P.
- Forsterd L.
- Renfrewb C.
- Forsterc M.
Phylogenetic network analysis of SARS-CoV-2 genomes.
PNAS. April 28, 2020; 117 ([first published April 8, 2020]): 9241-9243https://doi.org/10.1073/pnas.2004999117
Unlike in previous studies, we present here a case cluster of seven patients with COVID-19 with different genetic specifications whose infection was from the same point of origin. The similar and different clinical, radiological and laboratory findings of patients residing in the same nursing home and in the same age group, who presented to the hospital together 1 week after a suspicious contact, were evaluated. The aim of the study is thus to define the characteristics of COVID-19 that developed after transmitting from the same source to individuals in the same age group but with a different genetic pool.
2. Findings - case presentation
Presented in this study are seven cases, comprising four males and three females, with an age range of 78–91 years. Case 1 presented to our hospital with complaints of fever, cough and diarrhea on March 12, 2020, prior to COVID-19 being declared an epidemic in Turkey, with cases reported only in Istanbul. The children of Case 1, who had travelled from a country where the disease had been declared an epidemic, are known to have visited Case 1 prior to the onset of symptoms. There were also contacts with other residents of the nursing home during this visit. Case 1, who had no other contact history, underwent tests in the emergency service, in which a ground-glass appearance was noted in diffuse peripheral locations in bilateral lungs, and was hospitalized with the diagnosis of atypical pneumonia and suspicious COVID-19. Since the case was resident of a nursing home where communal living was the norm, cases with similar symptoms were asked to be brought for testing by officials, and a total of six other symptomatic cases presented to the emergency service that night and the following day. The body temperatures of two patients were found to be high at admission, and it was learned that all cases had developed a fever over the last 48 h. All patients had a dry cough and Case 1 had also a cough with sputum occasionally; furthermore four cases had diarrhea and four had dyspnea at admission, while only one complained of vomiting. The general characteristics of the patients and vital signs at admission are presented in Table 1.
Table 1General demographics characteristics and vital signs of cases at presentation.
| Sex | Age | Application complaint | Fever (°C) | ABP (mmHg) | Pulse (/min) | RR (/min) | SpO2 (%) | |
|---|---|---|---|---|---|---|---|---|
| Case 1 | M | 80 | Fever Dry cough Diarrhea Dyspnea | 38.9 | 160/80 | 105 | 28 | 92 |
| Case 2 | M | 83 | Fever Weakness Dry cough Diarrhea | 38 | 124/59 | 70 | 22 | 92 |
| Case 3 | F | 78 | Fever Dry cough Diarrhea | 36.4 | 112/48 | 110 | 20 | 91 |
| Case 4 | M | 87 | Fever Dry cough Vomiting | 36.4 | 153/68 | 90 | 22 | 91 |
| Case 5 | F | 91 | Fever Dry cough Dyspnea | 36.2 | 120/75 | 80 | 20 | 95 |
| Case 6 | F | 80 | Fever Dry cough Dyspnea | 37.4 | 100/50 | 88 | 20 | 90 |
| Case 7 | M | 85 | Fever Dry cough Dyspnea Diarrhea | 37.1 | 126/90 | 91 | 20 | 91 |
F: Female.
M: Male.
SpO2: Pulse oximeter oxygen saturation.
ABP: Arterial blood pressure.
RR: Respiratory rate.
HT: Hypertension.
ICU: Intensive care unit.
COPD: Chronic obstructive pulmonary disease.
CHF: Congestive heart failure.
HL: Hyperlipidemia.
CRF: Chronic renal failure.
DM: Diabetes mellitus.
HB: Heart block.
CAD: Coronary artery disease.
All seven patients had at least one chronic disease and five had hypertension. Cases 5, 6 and 7 had more than three chronic diseases. A thoracic computed tomography (CT) of the patients revealed a dominant picture of a bilateral peripheral ground-glass opacity in multiple foci. Lung involvement was unilateral only in Cases 4 and 5, but with multiple foci. The comorbidities and CT results of the patients are presented in Table 2.
Table 2The relationship between radiological imaging, medical history, comorbidity and clinical outcome of cases.
| Comorbidity | Medication | Thorax CT | |
|---|---|---|---|
| Case 1 | HT CAD | Telmisartan Clopidogrel Acetylsalicylic acid Solifenacin succinate Vitamin complex B1-B6-B12 |  |
| Case 2 | CAD COPD | Ramprril Tiotropium bromide monohydrate |  |
| Case 3 | HT | Not using medication | 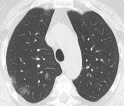 |
| Case 4 | HT HB and Pacemaker | Levotyroxin sodium Clopidogrel Atorvastatin Valsartan + hydrochlorothiazide Trimetazidine | 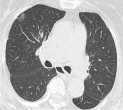 |
| Case 5 | HT Alzheimer's disease Major depression | Memantine Acetylsalicylic acid Amlodipine Donozepile Trazodone | 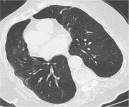 |
| Case 6 | Alzheimer's disease CAD CHF COPD | Ipratropium bromide monohydrate + salbutamol sulfate Paroksetine Salmoterole + flutikazone Metoprolol Losartan Trimetazidine Benidipine hydrochloride Memantine + donepezil |  |
| Case 7 | Parkinson's disease COPD CHF HT, DM HL, CRF BPH AF | Acetylsalicylic acid Piribedil Amiodarone Trimetazidine Gabapentin Dutasteride Tamsulosin hydrochloride Piracetam |  |
HT: Hypertension.
ICU: Intensive care unit.
COPD: Chronic obstructive pulmonary disease.
CHF: Congestive heart failure.
HL: Hyperlipidemia.
CRF: Chronic renal failure.
DM: Diabetes mellitus.
HB: Heart block.
CAD: Coronary artery disease.
CHF: Congestive heart failure.
AF: Atrial fibrillation.
BPH: Benign prostatic hypertrophy.
White blood cell (WBC) and neutrophil counts were within normal ranges at presentation to the emergency room in all patients. Lymphopenia was present in Cases 1, 2, 4 and 7. Also Cases 1, 2 and 7 had thrombocytopenia, and Cases 4 and 5 were identified with thrombocytopenia during follow-up. The C-reactive protein (CRP) level was higher than normal in all patients. Procalcitonin was slightly high in Cases 2, 3 and 6. Albumin was within the normal range only in Cases 1 and 4 initially, being low in all other cases, while hypoalbuminemia was seen in all patients during follow-up. Other laboratory findings were presented in Table 3.
Table 3Laboratory findings of cases.
| WBC (10^9/L) | Hgb (g/dl) | N (10^9/L) | L (10^9/L) | PLT (10^9/L) | CRP (mg/L) | Procalcitonin (ug/L) | Cr (mg/dL) | Albumin (g/L) | LDH (U/L) | CK-MB (ug/L) | Trp I (ng/ML) | AST (U/L) | ALT (U/L) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 4.48 | 11.5 | 3.53 | 0.73 | 105 | 46 | 0.05 | 1.5 | 38 | 34 | 17 | |||
| 3.66 | 11.5 | 2.42 | 0.83 | 149 | 74 | 1.4 | 458 | 13.6 | 0 | 58 | 19 | |||
| 4.45 | 10.3 | 3.27 | 0.69 | 229 | 96 | 0.04 | 1.2 | 34 | 9.4 | 0 | 38 | 18 | ||
| 7.52 | 11.4 | 5.25 | 1.60 | 381 | 14 | 0.01 | 1.3 | 1.6 | 0 | 19 | 17 | |||
| 6.94 | 12.4 | 4.57 | 1.67 | 376 | 24 | 1.5 | 17 | 17 | ||||||
| Case 2 | 7.54 | 11.5 | 6.65 | 0.33 | 105 | 144 | 0.21 | 1.1 | 31 | 36 | 23 | |||
| 4.85 | 13 | 3.86 | 0.55 | 226 | 155 | 1.0 | 5.65 | 0.09 | 28 | 18 | ||||
| 5.77 | 13.2 | 4.36 | 0.67 | 316 | 101 | 0.10 | 1.1 | 31 | 2.24 | 0.04 | 21 | 19 | ||
| 6.47 | 12.9 | 4.66 | 0.79 | 289 | 90 | 0.9 | 1.55 | 0.02 | 22 | 21 | ||||
| 5.59 | 12.5 | 3.81 | 0.92 | 389 | 70 | 0.01 | 0.91 | 34 | 164 | 22 | 24 | |||
| 5.10 | 12.4 | 3.53 | 0.79 | 314 | 24 | 0.11 | 0.94 | 20 | 23 | |||||
| 4.73 | 12.7 | 2.87 | 1.11 | 374 | 15 | 0.01 | 1.09 | 36 | 138 | 16 | 18 | |||
| Case 3 | 6.75 | 10.4 | 4.89 | 1.23 | 197 | 68 | 0.15 | 1.27 | 21 | 13 | ||||
| 5.30 | 9.9 | 4.07 | 0.94 | 182 | 70 | 1.24 | 34 | 155 | 0.62 | 0 | 19 | 13 | ||
| 4.92 | 9.9 | 3.4 | 1.18 | 229 | 50 | 0.14 | 1.04 | 48 | 29 | |||||
| 6.73 | 10.7 | 5.25 | 1.03 | 333 | 0.06 | 0.14 | 0 | |||||||
| 5.45 | 10.5 | 3.89 | 1.04 | 271 | 67 | 0.01 | 1.03 | 33 | 37 | |||||
| 6.36 | 10.3 | 4.13 | 1.03 | 492 | 39 | 1.08 | 33 | 22 | 23 | |||||
| 4.35 | 10.3 | 2.71 | 1.39 | 450 | 9.4 | 0.05 | 0.86 | 42 | 39 | |||||
| Case 4 | 7.64 | 11.9 | 5.60 | 0.51 | 244 | 8.8 | 0.02 | 0.87 | 41 | 26 | 17 | |||
| 6.25 | 12 | 2.66 | 1.61 | 190 | 10.8 | 1 | 40 | 201 | 0.61 | 0.01 | 21 | 17 | ||
| 5.14 | 11.2 | 2.67 | 2.37 | 126 | 15 | 0.01 | 0.84 | |||||||
| 8.04 | 11.7 | 4.37 | 2.50 | 323 | 6.7 | 0.01 | 1.05 | 16 | 14 | |||||
| 9.73 | 11.5 | 6.61 | 1.95 | 346 | 12 | 0.98 | 17 | 12 | ||||||
| 8.14 | 11.1 | 5.11 | 1.87 | 324 | 4.6 | 0.01 | 0.88 | 34 | 11 | 9 | ||||
| Case 5 | 7.38 | 14.6 | 4.50 | 1.70 | 161 | 76 | 0.09 | 1.37 | 32 | 18 | 11 | |||
| 4.92 | 13.5 | 2.94 | 1.37 | 139 | 0.51 | 13 | 6 | |||||||
| 4.56 | 13.8 | 2.74 | 1.19 | 182 | 78 | 0.09 | 0.78 | 0.01 | ||||||
| 4.09 | 13.1 | 2.67 | 0.97 | 121 | 0.63 | 32 | 25 | 13 | ||||||
| 4.51 | 13.2 | 2.93 | 1.01 | 148 | 58 | |||||||||
| 4.38 | 12.3 | 2.80 | 0.91 | 117 | ||||||||||
| 5.10 | 12.8 | 3.24 | 0.90 | 133 | 93 | |||||||||
| 5.90 | 12.5 | 4.04 | 0.99 | 175 | 28 | 21 | ||||||||
| 12.1 | 13.6 | 9.97 | 0.86 | 234 | 125 | 0.74 | 8.26 | 0.47 | 33 | 25 | ||||
| Case 6 | 7.55 | 10.6 | 5.25 | 1.24 | 204 | 46 | 0.11 | 1.99 | 32 | 43 | 24 | |||
| 11.3 | 10.2 | 9.25 | 1.24 | 288 | 111 | 1.59 | 229 | 1.39 | 0.03 | 33 | 27 | |||
| Case 7 | 6.24 | 11.9 | 5.01 | 0.73 | 134 | 158 | 0.1 | 1.24 | 34 | 30 | 34 | |||
| 5.14 | 12.7 | 4.42 | 0.39 | 151 | 129 | 1.48 | 71 | 55 | ||||||
| 4.65 | 12.3 | 3.96 | 0.57 | 165 | 143 | 0.1 | 1.27 | 33 | 401 | 15.6 | 0.01 | 77 | 61 | |
| 6.66 | 11.9 | 5.83 | 0.49 | 192 | 143 | 0.1 | 1.3 | 102 | 77 |
Laboratory results are presented one after the other for each case in order of date.
Reference ranges of laboratory tests
Lymphocyte: 0.8–4 10^9/L.
Platelet: 150–400 10^9/L.
C-reaktif protein: 0–5 mg/L.
Procalcitonin: 0–0.1 μg/L.
Albumin: 35–50 g/L.
Creatinine: 0.7–1.3 mg/dL.
Aspartat aminotransferaz: 5–35 U/L.
Alanin aminotransferaz: 0–55 U/L.
Troponin: 0–0.06 ng/mL.
Creatine kinase-myocardial isoenzyme: 0–5 μg/L.
Lactate dehydrogenase: 125–220 U/L.
Abbreviations:
N: Neutrophil.
L: Lymphocyte.
WBC: White blood cell count.
Hgb: Hemoglobin.
PLT: Platelet.
CRP: C-reaktif protein.
Cr: Creatinine.
Trp: Troponin.
CK-MB: Creatine kinase-myocardial isoenzyme.
AST: Aspartat aminotransferaz.
ALT: Alanin aminotransferaz.
LDH: Lactate dehydrogenase.
For the electrolytes of the patients, Sodium (Na+) was low only in Case 6 initially, while moderate hyponatremia developed in Case 7 during follow-up. Abnormal potassium (K+) values were seen only in Cases 2 and 5, who were hypokalemic. Calcium (Ca+) levels were within the normal range only in Cases 3 and 4 at presentation, while low in the rest of the cases, and hypocalcemia persisted despite treatment during the follow-up. The follow-up of electrolyte levels of the patients is presented in Table 4.
Table 4Blood gases analysis and electrolytes of patients.
| pH | PCO2 (mmHg) | PO2 (mmHg) | HCO3 (mmol/L) | BE-ECF (mmol/L) | Lactate (mmol/L) | SO2 (%) | Na+ (mmol/L) | K+ (mmol/L) | Ca+ (mg/dL) | Clinical outcome | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 7.39 | 32 | 68 | 20 | −5.6 | 95 | 135 | 4.7 | 7.7 | Discharged | |
| 0.5 | 137 | 4.2 | |||||||||
| 7.41 | 33 | 111 | 22 | −3.3 | 1 | 97 | 135 | 4.2 | 8.7 | ||
| 7.33 | 50 | 90 | 22 | 0.7 | 2 | 95 | 137 | 4.8 | |||
| 138 | 4.4 | ||||||||||
| Case 2 | 7.52 | 30 | 80 | 27 | 1.6 | 0.9 | 96 | 135 | 2.7 | 7.7 | Discharged |
| 7.43 | 45 | 56 | 27 | 5.9 | 1.3 | 84 | 141 | 3.3 | |||
| 135 | 3.1 | 7.7 | |||||||||
| 136 | 3.7 | ||||||||||
| 136 | 4 | 8.2 | |||||||||
| 7.43 | 39 | 78 | 26 | 2.1 | 0.9 | 95 | 135 | 4.3 | |||
| 139 | 4.8 | 8.5 | |||||||||
| Case 3 | 7.41 | 39 | 79 | 25 | 0.3 | 0.7 | 96 | 134 | 4.1 | 9.4 | Discharged |
| 7.14 | 60 | 44 | 17 | −7.9 | 0.8 | 58 | 138 | 4.1 | |||
| 7.38 | 48 | 70 | 25 | 3.3 | 1.2 | 89 | 137 | 4.6 | |||
| 7.49 | 32 | 95 | 26 | 1.3 | 1.1 | 97 | |||||
| 7.39 | 22 | 144 | 16 | −10.8 | 1.0 | 110 | 141 | 4.2 | |||
| 7.50 | 23 | 81 | 23 | −4.3 | 1.1 | 96 | |||||
| 7.52 | 29 | 83 | 26 | 1.1 | 1.0 | 96 | 140 | 3.9 | |||
| 138 | 4.3 | 10.1 | |||||||||
| Case 4 | 7.45 | 38 | 53 | 27 | 2.7 | 1.1 | 90 | 139 | 4.3 | 9.8 | Discharged |
| 7.48 | 35 | 61 | 27 | 2.2 | 0.8 | 94 | |||||
| 7.39 | 46 | 54 | 25 | 2.9 | 0.9 | 84 | 141 | 4.2 | 9.3 | ||
| 141 | 4.6 | 9.4 | |||||||||
| 145 | 4.7 | 9.3 | |||||||||
| 145 | 4.6 | ||||||||||
| Case 5 | 7.41 | 37 | 62 | 24 | −0.8 | 1.1 | 97 | 141 | 4.6 | 8.1 | Dead at ICU |
| 7.39 | 42 | 223 | 25 | 0.6 | 0.8 | 99 | 146 | 2.7 | 7.2 | ||
| 7.38 | 44 | 61 | 25 | 1.2 | 0.7 | 92 | 140 | 6.2 | |||
| 7.47 | 35 | 61 | 27 | 2 | 0.8 | 95 | 144 | 3.9 | 7.2 | ||
| 7.36 | 40 | 85 | 23 | −2.1 | 2.2 | 95 | 2.9 | ||||
| 7.35 | 27 | 86 | 18 | −9.9 | 3.8 | 97 | 144 | 3 | 7.3 | ||
| 144 | 3.4 | ||||||||||
| Case 6 | 7.41 | 35 | 110 | 22 | −2.5 | 1.2 | 96 | 129 | 4.5 | 8.0 | Dead at ICU |
| 7.31 | 36 | 60 | 19 | −7.2 | 0.8 | 90 | |||||
| 138 | 4 | 8.0 | |||||||||
| 7.41 | 31 | 53 | 21 | −4.3 | 1.4 | 83 | |||||
| Case 7 | 7.44 | 32 | 59 | 23 | −2.2 | 0.6 | 92 | 135 | 4.4 | 8.2 | Dead at ICU |
| 7.34 | 38 | 62 | 18 | −5.1 | 2.3 | 86 | 135 | 4.2 | |||
| 7.27 | 26 | 61 | 14 | −14.3 | 1.7 | 86 | 134 | 3.8 | 8.2 | ||
| 7.26 | 26 | 61 | 13 | −14.3 | 1.7 | 86 | 132 | 4.1 | |||
| 7.29 | 29 | 48 | 15 | −11.5 | 4.5 | 70 |
Laboratory results are presented one after the other for each case in order of date.
Reference ranges of laboratory tests
Sodium: 135–146 mmol/L.
Potassium: 3.5–5.5 mmol/L.
Calcium: 8.5–10.5 mg/dL.
Abbreviations:
pH: power of hydrogen.
PCO2: Partial pressure of carbon dioxide and oxygen.
PO2: Partial pressure of oxygen.
HCO3: Bicarbonate.
BE-ECF: base excess in the extracellular fluid compartment.
SO2: Oxygen Saturation.
Na+: Sodium.
K+: Potassium.
Ca+: Calcium.
An evaluation of the blood gas data of the patients revealed mostly a mixed type acid-base abnormality at least once in all patients. Mixed type acidosis was seen in Cases 1, 3, 5 and 7 and a simple type acidosis was seen in Case 6 at least once. A mixed type alkalosis was seen at least once during follow-up in Cases 2, 3, 4 and 5. No lactate level higher than 4.5 was seen in any of the patients during follow-up. A complete follow-up of blood gases of the patients is presented in Table 4.
The blood type of the patients was as follows: Case 1 and 2 A Rh (+), Case 3 A Rh (−), Case 4 0 Rh (−), (+), Case 5 and 6 AB Rh (+), and Case 7 0 Rh (+). Real time PCR test results were positive for SARS-CoV-2 in all seven patents after repeated measurements. All patients were hospitalized, and all were initially followed-up in the wards. The initial treatment was oral hydroxychloroquine, moxifloxacin and oseltamivir. Ritonavir 50 mg and lopinavir 200 mg orally was added to the treatment in Cases 5, 6 and 7, since the expected response to the initial treatment could not be obtained. All patients needed oxygen therapy. Cases 1, 2, 3 and 4 were discharged from the hospital after on day 16, day 16, day 17 and day 12 respectively of treatment; Cases 5, 6 and 7 were intubated following the development of severe and rapid respiratory failure on day 10, day 6 and day 5 respectively, and all died in three days after intubation.
3. Discussion
The genotype and phenotype of the host has been suggested to be influential in the course of COVID-19, as with many viral infections, although this suggestion is still speculative, or at a level of review [
13
,14
], and no serious genetic research has yet been concluded. Almost all studies evaluating the course of COVID-19 on similar genetic structures are of family clusters [9
, - Qian G.
- Yang N.
- Yan Ma A.H.
- et al.
COVID-19 transmission within a family cluster by presymptomatic carriers in China.
Clin Infect Dis. 2020; https://doi.org/10.1093/cid/ciaa316
10
, 11
]. However, although the genetic structure of the participants is similar in those studies, it is highly possible that the origin of the infection is the same, since they are from the same family and so may have transmitted the virus from one to the other. As in all viruses, SARS-CoV-2 can also undergo behavioral and genetic changes while changing the host, and the generation of subtypes may also be possible. And finally, Forster et al. showed three subtypes of the novel corona virus in their study [- Li P.
- Fu J.B.
- Li K.F.
- et al.
Transmission of COVID-19 in the terminal stage of incubation period: a familial cluster.
Int J Infect Dis. Mar 16, 2020; ([S1201 9712(20)30146-6])https://doi.org/10.1016/j.ijid.2020.03.027
12
]. However, there is no other study in the case of whether there are more subtypes. In a novel approach, the present study evaluates individuals with different genetic properties but of similar age who contracted the disease from the same source. As such, it is the first study to evaluate whether origin has a role in the disease.- Forster P.
- Forsterd L.
- Renfrewb C.
- Forsterc M.
Phylogenetic network analysis of SARS-CoV-2 genomes.
PNAS. April 28, 2020; 117 ([first published April 8, 2020]): 9241-9243https://doi.org/10.1073/pnas.2004999117
All cases were similar in terms of age in this case cluster of seven individuals who contracted the disease from the same host. All patients developed fever and dry cough as symptoms. Worthy of note, four had diarrhea. Fever, cough and diarrhea have been reported in previous studies in rages of 44–98%, 67–76% and 3–4%, respectively [
6
,- Guan W.
- Ni Z.
- Hu Yu
- Liang W.
- et al.
Clinical characteristics of coronavirus disease 2019 in China.
N Engl J Med. Feb 28, 2020; https://doi.org/10.1056/NEJMoa2002032
7
,15
]. Dyspnea was seen in four of the patients in the present study, three of whom died. The most correlated factor with mortality was dyspnea at admission (Table 1). Complaints at admission were different from those reported in literature, but similar within the patient group.- Chen D.
- Li X.
- Song Q.
- et al.
Hypokalemia and clinical implications in patients with coronavirus disease 2019 (COVID-19).
https://www.medrxiv.org/content/10.1101/2020.02.27.20028530v1
Date: Feb 29, 2020
Date accessed: March 12, 2020
One of the factors most correlated with mortality in this case series was chronic disease and the number of chronically used drugs. All patients with three or more chronic diseases died. In this respect, the findings related to this case cluster resembled those reported in literature [
6
,- Guan W.
- Ni Z.
- Hu Yu
- Liang W.
- et al.
Clinical characteristics of coronavirus disease 2019 in China.
N Engl J Med. Feb 28, 2020; https://doi.org/10.1056/NEJMoa2002032
16
]. The possibility of mortality increased with the increase in the number of drugs used. In addition, as a specific point, three out of four patients on Ca+ canal blockers died. The number of patients of angiotensin-converting enzyme inhibitors, angiotensin receptor blockers and anti-platelets were similar in the groups of patients that died and survived (Table 2).When the case cluster was examined radiologically, five out of seven cases had bilateral involvement, and all had peripherally located ground-glass opacity in multiple foci. The rate of bilateral involvement and ground glass opacity was reported to be 51% and 56%, respectively in a previously published extensive case series [
6
]. The present case series, involving patients who contracted the disease from the same source, is different from previous in this respect, while similar characteristics were observed within the case series itself.- Guan W.
- Ni Z.
- Hu Yu
- Liang W.
- et al.
Clinical characteristics of coronavirus disease 2019 in China.
N Engl J Med. Feb 28, 2020; https://doi.org/10.1056/NEJMoa2002032
When the laboratory data of the patients in this present series is compared with the results of other studies, the number of patients with lymphopenia, thrombocytopenia, hypoalbuminemia, elevated LDH and ALT was similar compared to other studies, while the number of patients with AST and CRP elevation, hypokalemia and hypocalcemia was significantly different when compared to other studies [
6
,- Guan W.
- Ni Z.
- Hu Yu
- Liang W.
- et al.
Clinical characteristics of coronavirus disease 2019 in China.
N Engl J Med. Feb 28, 2020; https://doi.org/10.1056/NEJMoa2002032
7
,15
]. Lymphopenia was present in four out of seven patients in the present case cluster. All patients with an increase in the lymphocyte count, regardless of whether or not the initial lymphocyte count was within normal ranges, survived, and all patients whose lymphocyte counts decreased or stayed the same during follow-up died. Platelet counts tended to be elevated in all patients with treatment, regardless of the clinical outcome. The drugs administered to the patients did not cause thrombocytosis, although it has been suggested that hydroxychloroquine may cause thrombocytopenia []. As such, another common feature in these patients that may have caused an increased platelet count is the presence of COVID-19. The underlying cause of increased D-Dimer [- Chen D.
- Li X.
- Song Q.
- et al.
Hypokalemia and clinical implications in patients with coronavirus disease 2019 (COVID-19).
https://www.medrxiv.org/content/10.1101/2020.02.27.20028530v1
Date: Feb 29, 2020
Date accessed: March 12, 2020
6
] and coagulation tendency [- Guan W.
- Ni Z.
- Hu Yu
- Liang W.
- et al.
Clinical characteristics of coronavirus disease 2019 in China.
N Engl J Med. Feb 28, 2020; https://doi.org/10.1056/NEJMoa2002032
18
] in patients with COVID-19 may be the gradual increase in platelet count. CRP was increased in all patients in this case cluster. CRP levels were increased more on days 2 and 3 of treatment in six out of the seven cases. Cases 1,2, 3 and 4, in which the CRP levels were gradually decreased, all survived, while cases 5, 6 and 7, in which no gradual decrease was noted, all died. Chen et al. reported previously that 62% of their patient population of COVID-19 had hypokalemia, and so they associated non-responding or advancing hypokalemia with mortality [15
]. Only one of the patients in the present study had hypokalemia initially, while one developed hypokalemia during clinical follow-up. Of these, one patient survived and the other died. Hypocalcemia was dominant among the patients in the present series, with five out of the seven patients identified with hypocalcemia initially. Among these patients, those whose calcium (Ca+) levels improved with treatment survived, while those with a decrease or no increase in calcium levels, despite treatment, died.- Chen D.
- Li X.
- Song Q.
- et al.
Hypokalemia and clinical implications in patients with coronavirus disease 2019 (COVID-19).
https://www.medrxiv.org/content/10.1101/2020.02.27.20028530v1
Date: Feb 29, 2020
Date accessed: March 12, 2020
When the acid-base metabolism of the patients was evaluated, none of the deep acidosis or high lactate levels that we are used to seeing prior to the death of patients were observed. It is possible to say that clinical deterioration and death occurred prior to impairment of the laboratory data when the metabolic data were close to normal ranges. An initial negative BE-ECF value, namely a susceptibility to acidosis, is associated more with mortality. Three out of four patients with an initial negative BE-ECF died. We could identify no studies presenting blood gas values in detail to allow a comparison with our results.
It is seen that the findings related to this case cluster of patients with the same source of infection differ from those in literature in such parameters as complaints at admission, radiological imaging, clinical outcome and laboratory data, while having similar characteristics within the cluster itself. In addition, it was noted that patients with Ca canal blocker use, hypocalcemia and negative BE-ECF may carry a higher risk of mortality. Furthermore, lymphocyte count and CRP seem to be useful in the follow-up of response to treatment.
4. Conclusion
The complaints at presentation, and the laboratory and radiological data of patients with COVID-19 who contracted the disease from the same host, are different from those in literature, but similar within the patient cluster. This suggests that subtypes of the new coronavirus may exist and cause different clinical courses. Therefore, the origin of infection may aid in predicting the course in a patient with COVID-19. Detecting mild subtypes can be useful in developing a vaccine against Covid-19.
Acknowledgements
We would like to thank our patient who allowed us to take photos and share them for medical purposes.
Ethical approval
This is a case report. For this reason, consent was obtained from the relevant persons for sharing the data, but the ethical committee approval was not obtained because it did not require ethical committee approval.
Human rights
Human rights were observed in the study and the Helsinki Declaration was followed.
Declaration of competing interest
The authors had no conflicts of interest to declare in relation to this article.
References
- Coronavirus disease (COVID-2019) situation reports.([Available at 24 April 2020])
- The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak - an update on the status.Mil Med Res. Mar 13, 2020; 7: 11
- WHO declares COVID-19 a pandemic.Acta Biomed. Mar 19, 2020; 91: 157-160
- The COVID-19 epidemic.Trop Med Int Health. Mar 2020; 25: 278-280
- Chest CT findings in cases from the cruise ship “diamond princess” with coronavirus disease 2019 (COVID-19).Cardiothorac Imaging. Mar 17, 2020; 2https://doi.org/10.1148/ryct.2020200110
- Clinical characteristics of coronavirus disease 2019 in China.N Engl J Med. Feb 28, 2020; https://doi.org/10.1056/NEJMoa2002032
- Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China.Lancet. 2020; 395: 497-506
Zhao J, Yang Y, Huang H, et al. Relationship between the ABO blood group and the COVID-19 susceptibility. medRxiv 2020.03.11.20031096; doi:https://doi.org/10.1101/2020.03.11.20031096.
- COVID-19 transmission within a family cluster by presymptomatic carriers in China.Clin Infect Dis. 2020; https://doi.org/10.1093/cid/ciaa316
- A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster.Lancet. 2020; 395: 514-523
- Transmission of COVID-19 in the terminal stage of incubation period: a familial cluster.Int J Infect Dis. Mar 16, 2020; ([S1201 9712(20)30146-6])https://doi.org/10.1016/j.ijid.2020.03.027
- Phylogenetic network analysis of SARS-CoV-2 genomes.PNAS. April 28, 2020; 117 ([first published April 8, 2020]): 9241-9243https://doi.org/10.1073/pnas.2004999117
- Initial review and analysis of COVID-19. Host genetics and associated phenotypes.Preprints, 2020 ([2020030356])
- 23andMe to study genetic factors of COVID-19 severity using data from consented customers.(Available)
- Hypokalemia and clinical implications in patients with coronavirus disease 2019 (COVID-19).https://www.medrxiv.org/content/10.1101/2020.02.27.20028530v1Date: Feb 29, 2020Date accessed: March 12, 2020
- Characteristics of COVID-19 patients dying in Italy. Report based on available data on March 20th, 2020.(Available)
- Hydroxychloroquine: drug information.(Available)
- COVID-19 associated thrombotic complications.(Available)
Article Info
Publication History
Published online: June 01, 2020
Accepted:
May 29,
2020
Received:
May 20,
2020
Identification
Copyright
© 2020 Elsevier Inc. All rights reserved.
