



Abstract
Background
We report a patient with a massive hydroxychloroquine overdose manifested by profound
hypokalemia and ventricular dysrhythmias and describe hydroxychloroquine toxicokinetics.
Case report
A 20-year-old woman (60 kg) presented 1 h after ingesting 36 g of hydroxychloroquine.
Vital signs were: BP, 66 mmHg/palpation; heart rate, 115/min; respirations 18/min;
oxygen saturation, 100% on room air. She was immediately given intravenous fluids
and intubated. Infusions of diazepam and epinephrine were started. Activated charcoal
was administered. Her initial serum potassium of 5.3 mEq/L decreased to 2.1 mEq/L
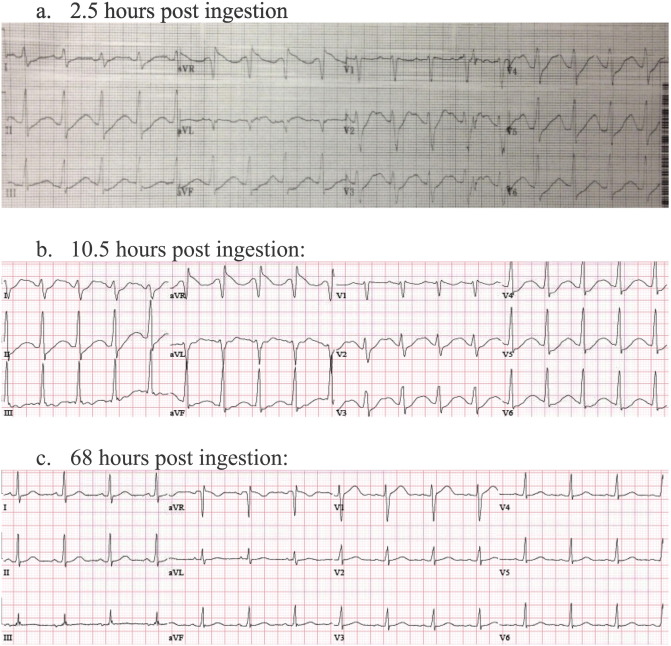
1 h later. The presenting electrocardiogram (ECG) showed sinus tachycardia at 119
beats/min with a QRS duration of 146 ms, and a QT interval of 400 ms (Bazett's QTc
563 ms). She had four episodes of ventricular tachydysrhythmias requiring cardioversion,
electrolyte repletion, and lidocaine infusion. Her blood hydroxychloroquine concentration
peaked at 28,000 ng/mL (therapeutic range 500–2000 ng/mL). Serial concentrations demonstrated
apparent first-order elimination with a half-life of 11.6 h. She was extubated on
hospital day three and had a full recovery.
Conclusion
We present a massive hydroxychloroquine overdose treated with early intubation, activated
charcoal, epinephrine, high dose diazepam, aggressive electrolyte repletion, and lidocaine.
The apparent 11.6 hour half-life of hydroxychloroquine was shorter than previously
described.
To read this article in full you will need to make a payment
Subscribe to The American Journal of Emergency Medicine
Already a print subscriber? Claim online access
Already an online subscriber? Sign in
Register: Create an account
Institutional Access: Sign in to ScienceDirect
References
- Treatment of severe chloroquine poisoning.N Engl J Med. 1988; 318: 1-6
- Protective cardiovascular effects of diazepam in experimental acute chloroquine poisoning.Intensive Care Med. 1988; 14: 610-616
- Hydroxychloroquine overdosage.J Rheumatol. 1989; 16: 142-143
- Hydroxychlorouine kinetics after overdose (abstract).J Toxicol Clin Toxicol. 1997; 35: 496
- Hydroxychloroquine overdose: toxicokinetics and management.J Toxicol Clin Toxicol. 1999; 37: 861-864
- Therapy and pharmacological properties of hydroxychloroquine and chloroquine in treatment of systemic lupus erythematosus, rheumatoid arthritis and related diseases.Inflammopharmacology. 2015; 23: 231-269
- A dose-ranging study of the pharmacokinetics of hydroxy-chloroquine following intravenous administration to healthy volunteers.Br J Clin Pharmacol. 1988; 26: 303-313
- Prevention of chloroquine absorption by activated charcoal.Hum Exp Toxicol. 1992; 11: 117-120
- Clinical pharmacokinetics of slow-acting antirheumatic drugs.Clin Pharmacokinet. 1993; 25: 392-407
- Pharmacokinetics of hydroxychloroquine and its clinical implications in chemoprophylaxis against malaria caused by Plasmodium vivax.Antimicrob Agents Chemother. 2009; 53: 1468-1475
- Antimalarial 4-aminoquinolines: mode of action and pharmacokinetics.Fundam Clin Pharmacol. 1994; 8: 1-17
- Hypokalaemia related to acute chloroquine ingestion.Lancet. 1995; 346: 877-880
- Clinical features and management of poisoning due to antimalarial drugs.Med Toxicol Adverse Drug Exp. 1987; 2: 242-273
- Hydroxychloroquine and cardiotoxicity: a retrospective review of regional poison center data.Clin Toxicol. 2013; 51: 712
- Hydroxychloroquine poisoning and the potential for cardiotoxicity [abstract], ACMT 2018 annual scientific meeting abstracts-Washington, DC.J Med Toxicol. 2018; : 3-67
- Novel therapies for myocardial irritability following extreme hydroxychloroquine toxicity.Case Rep Emerg Med. 2015; 2015: 692948
- Early treatment with intravenous lipid emulsion in a potentially lethal hydroxychloroquine intoxication.Neth J Med. 2016; 74: 210-214
Article Info
Publication History
Published online: August 06, 2019
Accepted:
August 5,
2019
Received:
June 19,
2019
Identification
Copyright
© 2019 Elsevier Inc. All rights reserved.
