If you don't remember your password, you can reset it by entering your email address and clicking the Reset Password button. You will then receive an email that contains a secure link for resetting your password
If the address matches a valid account an email will be sent to __email__ with instructions for resetting your password
Acute chloroquine and hydroxychloroquine toxicity is characterized by a combination of direct cardiovascular effects and electrolyte derangements with resultant dysrhythmias and is associated with significant morbidity and mortality.
Objective
This review describes acute chloroquine and hydroxychloroquine toxicity, outlines the complex pathophysiologic derangements, and addresses the emergency department (ED) management of this patient population.
Discussion
Chloroquine and hydroxychloroquine are aminoquinoline derivatives widely used in the treatment of rheumatologic diseases including systemic lupus erythematosus and rheumatoid arthritis as well as for malaria prophylaxis. In early 2020, anecdotal reports and preliminary data suggested utility of hydroxychloroquine in attenuating viral loads and symptoms in patients with SARS-CoV-2 infection. Aminoquinoline drugs pose unique and significant toxicological risks, both during their intended use as well as in unsupervised settings by laypersons. The therapeutic range for chloroquine is narrow. Acute severe toxicity is associated with 10–30% mortality owing to a combination of direct cardiovascular effects and electrolyte derangements with resultant dysrhythmias. Treatment in the ED is focused on decontamination, stabilization of cardiac dysrhythmias, hemodynamic support, electrolyte correction, and seizure prevention.
Conclusions
An understanding of the pathophysiology of acute chloroquine and hydroxychloroquine toxicity and available emergency treatments can assist emergency clinicians in reducing the immediate morbidity and mortality associated with this disease.
Chloroquine and hydroxychloroquine are aminoquinoline derivatives widely used in the treatment of rheumatologic diseases as well as for malaria prophylaxis [
]. In early 2020, anecdotal reports and preliminary data suggested utility of chloroquine and hydroxychloroquine for attenuating viral loads and symptoms in patients with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection [
]. Shortly following publication of initial reports indicating efficacy, cases of acute chloroquine toxicity including inadvertent deaths were reported in the United States (U.S.), African, and European newsmedia [
]. There were 283 chloroquine and hydroxychloroquine exposures reported to U.S. Poison Control Centers from January 1, 2020 through April 26, 2020, an increase of 42% compared to the same time period during the previous year, with a 93% increase during the month of April 2020 when compared to April 2019 [
National Poison Data System (NPDS) Bulletin COVID-19 (Hydroxychloroquine/Chloroquine) [press release]. American Association of Poison Control Centers,
2020
]. Aminoquinoline drugs, including chloroquine, hydroxychloroquine, and amodiaquine, pose unique and significant toxicological risks, both in therapeutic use as well as in unsupervised settings by laypersons. For the purposes of this review, “aminoquinolines” will refer to chloroquine and hydroxychloroquine.
The therapeutic margin for chloroquine toxicity is narrow, and acute severe toxicity is associated with 10–30% mortality owing to a combination of direct cardiovascular effects and electrolyte derangements with resultant dysrhythmias [
]. In typical use, aminoquinoline toxicity is rarely reported. Fewer than 10 cases of acute severe chloroquine or hydroxychloroquine overdoses were reported to U.S. Poison Control Centers from 2012 to 2018, and approximately 70 cases of chloroquine or hydroxychloroquine overdose were reported in the literature base in the past decade [
]. While commonly prescribed for rheumatologic diseases, the novel proposed indication for SARS-CoV-2 infection represents an unprecedented expansion of aminoquinoline use in a significantly wider population [
]. Similar to other toxicological emergencies, randomized controlled trials and systematic reviews analyzing management approaches are absent. Prospective clinical trials evaluating treatment are also rare and date back to the 1980s and 1990s [
]. Updated treatment recommendations for aminoquinoline toxicity since the development of rescue modalities including intravenous lipid emulsion (ILE) and extracorporeal membrane oxygenation (ECMO) are lacking [
]. This article reviews the pathophysiology of aminoquinoline toxicity to provide guiding principles for management of acute complications. Understanding these complications and the approach to the management of electrolyte imbalances and hemodynamic instability is essential to optimizing patient care, especially following acute intoxication that may bring patients to the emergency department.
2. Methods
This review provides a focused evaluation of emergency department-based evaluation and treatment of aminoquinoline toxicity. The authors searched PubMed and Google Scholar for articles containing the key words “hydroxychloroquine” OR “aminoquinoline” OR “chloroquine” OR “quinolone” AND “toxicity” OR “poisoning” OR “adverse effects”. The PubMed search was conducted from database inception to April 5, 2020, yielding over 6300 articles. The first 200 articles in Google Scholar were also evaluated for inclusion. The literature search was restricted to studies published in English, with a focus on emergency medicine and critical care. Authors evaluated case reports and series, retrospective and prospective studies, systematic reviews and meta-analyses, and narrative reviews. Authors also reviewed guidelines and supporting citations of included articles. Articles were chosen based upon author consensus. When available, systematic reviews and meta-analyses were preferentially selected. These were followed sequentially by randomized controlled trials, prospective studies, retrospective studies, case reports, and other narrative reviews, when alternate data were not available. A total of 121 articles were selected for inclusion in this narrative review.
3. Discussion
3.1 Proposed aminoquinoline uses in coronavirus infection
Chloroquine and hydroxychloroquine are derivatives of quinine, derived from the bark of the Peruvian Cinchona tree. Chloroquine was synthesized in 1934 but shelved for years due to concerns for toxicity in human patients. Hydroxychloroquine sulfate was developed in 1946 in an effort to produce a less toxic chloroquine analog. Animal toxicological studies demonstrate hydroxychloroquine to be approximately 40% less toxic than chloroquine [
]. Initially indicated for antimalarial treatment and prophylaxis, chloroquine and analogs found new anti-inflammatory use in World War II. As millions of soldiers used it against malaria, military physicians observed improvement in inflammatory arthritis, leading to trials demonstrating aminoquinoline efficacy for rheumatologic conditions [
]. Antimalarial efficacy of chloroquine waned in the late 20th century, though it is still used for malarial prophylaxis in regions with susceptible Plasmodium strains. Chloroquine analogues have also been found to have metabolic, antithrombotic, antineoplastic, and antiviral effects, and have been hypothesized as targeted agents against coronavirus infection since the 2003 SARS outbreak [
Coronavirus disease 2019 (COVID-19), caused by SARS-CoV-2, is responsible for a major international pandemic with significant morbidity and mortality rates between 1.5 and 9% depending on the population investigated [
Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention.
]. The pathophysiology of SARS-CoV-2 includes but is not limited to cytokine dysregulation, direct cytopathic effects on respiratory tract epitheliocytes, and down-regulation of lung protective angiotensin converting enzyme resulting in diffuse alveolar damage and hypercoagulability [
]. Efforts to repurpose or develop targeted therapeutics for SARS-CoV-2 infection have included assessment of anti-inflammatory drugs such as corticosteroids and interleukin inhibitors, macrolide antibiotics such as azithromycin, and direct-acting antivirals such as protease inhibitors and adenosine analogs [
]. The utility of aminoquinolines in attenuating infection severity is hypothesized to derive from preventing SARS-CoV-2 binding to target receptors and inhibiting viral cell entry [
]. Chloroquine and hydroxychloroquine are concentrated within the endosome, where they are thought to modulate organelle pH, inhibiting autophagosome formation and impairing cleavage of the SARS-CoV-2 spike protein [
]. Additional hypothesized immunomodulatory effects in SARS-CoV-2 infection include downregulation of T-cell response and inflammatory cytokine storm that play a role in organ injury and acute respiratory distress syndrome [
]. Preliminary in-vitro data and clinical trials in China and France in early 2020 using chloroquine and hydroxychloroquine suggested anti-SARS-CoV-2 activity [
]. These clinical trials utilized chloroquine at dosages and treatment courses greater than those prescribed for antimalarial and rheumatologic indications, raising concern for toxicological implications in susceptible patients. Following the United States Food and Drug Administration emergency use authorization for chloroquine and hydroxychloroquine in the treatment of SARS-CoV-2, many additional clinical trials with randomization, blinding, and larger sample sizes were initiated to determine the benefit and risks. The largest of these studies, enrolling over 96,000 patients, initially demonstrated increased in-hospital mortality rates in patients treated with chloroquine or hydroxychloroquine [
]. However, that study has since been retracted due to concerns regarding veracity of the data and analyses conducted and inability to conduct an independent and private peer review [
]. Additional studies have demonstrated similar findings of increased mortality or did not find any evidence of prevention of primary endpoints, such as need for mechanical ventilation or death in patients treated with aminoquinolines [
Chloroquine diphosphate in two different dosages as adjunctive therapy of hospitalized patients with severe respiratory syndrome in the context of coronavirus (SARS-CoV-2) infection: Preliminary safety results of a randomized, double-blinded, phase IIb clinical trial (CloroCovid-19 Study).
]. As of June 2020, there are over 40 ongoing clinical trials actively assessing the efficacy of chloroquine or hydroxychloroquine, demonstrating continued interest in its role as a therapeutic agent for COVID-19. Furthermore, additional trials targeting frontline healthcare workers are underway to assess for the possible preventative action of these agents. The use of chloroquine or hydroxychloroquine sulfate in combination with other novel antiviral agents has been discouraged by the United States Food and Drug Administration, as recent in-vitro data demonstrating increasing concentrations of chloroquine phosphate reduced formation of activated remdesivir triphosphate in human bronchial epithelial cells, raising concerns that it may reduce the antiviral activity of this medication [
]. Widespread non-prescription use of aminoquinolines for either prophylaxis or treatment by laypersons in response to fears of COVID-19 raises significant and continued concern for unintended toxicity from overdose and/or drug-drug interactions.
3.2 Chloroquine and hydroxychloroquine toxicology
3.2.1 Metabolism and pharmacokinetics
Despite slight differences in chemical structure, chloroquine and hydroxychloroquine are similar in regard to both metabolism and toxicity [
Hydroxychloroquine is much less active than chloroquine against chloroquine-resistant plasmodium falciparum, in agreement with its physicochemical properties.
]. Following ingestion, the drugs are rapidly absorbed from the upper gastrointestinal (GI) tract and slowly redistribute to other compartments, eventually accumulating in erythrocytes, liver, lung, kidney, heart, muscle, and retinal tissue [
]. The combination of rapid absorption, high oral bioavailability, and slow redistribution prompts early peak serum levels post-ingestion which correlate with symptom severity in overdose [
]. Median lethal doses (LD50) for chloroquine and hydroxychloroquine in humans are unknown as most available mortality data are derived from case reports and case series. As little as 2–3 g of chloroquine may be fatal in adult patients, though the most commonly reported lethal dose in adults is 3–4 g [
]. Significant toxicity from hydroxychloroquine has been reported in patients with plasma levels ranging between 2.05 and 18.16 μmol/L (640 μg to 6100 μg/L) and fatalities with postmortem blood levels of 142.89 μmol/L (48,000 μg/L) and 309.62 μmol/L (104,000 μg/L) [
]. Intrinsic liver disease, such as hepatitis, alcoholism, or those taking additional medications metabolized by the same P450 isozymes can also modify chloroquine and hydroxychloroquine metabolism [
Therapy and pharmacological properties of hydroxychloroquine and chloroquine in treatment of systemic lupus erythematosus, rheumatoid arthritis and related diseases.
]. Following hepatic metabolism, aminoquinolines are mainly excreted renally (Table 1). A small percentage of the initial ingested quantity of chloroquine or hydroxychloroquine is excreted unchanged [
Chloroquine and hydroxychloroquine are distinct in terms of serum concentration required to produce toxicity, as chloroquine produces lethal effects at approximately 25% of the serum concentration of hydroxychloroquine [
]. However, both drugs have similar mechanisms of action. Aminoquinolines are pharmacologically diverse with activity on many distinct organ systems, cellular receptor sites, and intracellular organelles. This versatility contributes to the myriad uses of aminoquinolines from antimalarial prophylaxis to immunomodulation [
]. They behave as class IA antiarrhythmics with “Quinidine-like” effects, decreasing inotropy and producing characteristic electrocardiographic (ECG) changes [
]. Finally, aminoquinolines have the ability to bind to and inhibit ATP-dependent potassium channels on pancreatic β-cells leading to a similar mechanism of systemic release of insulin as is observed with sulfonylureas [
Acute aminoquinoline toxicity affects multiple organ systems. The following sections describe effects from acute and chronic toxicity. Many of the features of aminoquinoline toxicity are pertinent to ED care, particularly serum abnormalities and cardiac, respiratory, and neurologic phenomena. Others may occur following admission or discharge from the ED and become more relevant in the context of patient history, including otologic and ophthalmic sequelae. A summary of these findings is displayed in Table 2.
Table 2Organ toxicity and symptomatology of quinine and aminoquinolines.
Organ System
Acute Toxicity
Chronic Toxicity
Cardiovascular
Syncope Hypotension PR, QRS- and QT-interval prolongation Atrioventricular blocks Ventricular arrhythmias Torsades de pointes
Cardiomyopathy Biatrial and/or biventricular enlargement Concentric hypertrophy with restrictive features
Serum Abnormalities
Hypoglycemia Hypokalemia
Central nervous system
Headache Confusion and delirium Tonic clonic seizures Hallucinations Ataxia
]. Aminoquinolines produce multiple effects on cardiac electrical conduction via sodium and potassium channel inhibition and α1-adrenergic receptor antagonism as previously mentioned [
]. Similar to class I antiarrhythmics, aminoquinolines have a dose-dependent effect on the cardiac action potential, binding more avidly to ion channels and exerting greater sodium channel blockade [
]. Also similar to class IA antiarrhythmics is the dose-dependent ability of aminoquinolines to bind and inhibit the action of potassium channels. As potassium is responsible for myocyte repolarization, potassium channel blockade delays repolarization. Clinically, this produces additional QT prolongation and predisposes to torsades de pointes (TdP) [
Acute cardiac toxicity manifests as conduction blocks involving the atrioventricular junction and His-Purkinje system and ECG changes with prolongation in PR, QRS, and QT intervals [
]. Following overdose, these abnormalities can be profound, with reports of corrected QT (QTc) intervals of 563 milliseconds (ms) and 600 ms in case reports detailing oral hydroxychloroquine overdoses of 36 g and 22 g, respectively [
]. Patients with underlying prolonged QTc from structural heart disease, congenital long-QT syndromes, electrolyte disturbances, renal failure, and/or use of additional QT prolonging medications are at heightened risk for development of dysrhythmias including TdP [
]. Hydroxychloroquine induced conduction delay often presents as a progression from a singular fascicular block to bundle branch block, followed by third-degree AV block [
]. Secondary to α1-adrenergic blockade, acutely toxic patients present with hypotension, which in addition to dysrhythmias may cause presyncope or syncope [
While unlikely to occur in acute overdose, cardiomyopathy is described in case reports of patients presenting with chronic chloroquine and/or hydroxychloroquine toxicity [
]. Aminoquinoline-related cardiomyopathy has been reported with findings of biatrial and/or biventricular enlargement as well as concentric hypertrophy with restrictive features [
]. Chronic exposure to cumulative doses of 1277 g and 1843 g of chloroquine and hydroxychloroquine, respectively, over an average of 13 years has been demonstrated to produce this effect [
]. Risk of development is greater in patients with underlying heart failure or structural heart defects. Sequelae of drug-induced cardiomyopathy include acute and chronic heart failure, recurrent syncopal episodes, and newly developed conduction disorders [
]. Treatment-refractory hypokalemia is often one of the most challenging features following acute intoxication and is associated with cardiac manifestations including dysrhythmias [
]. Case reports from acute overdose report serum potassium concentrations of 2.5–2.7 mEq/L despite management with up to 280 mEq of potassium chloride [
]. The mechanism underlying hypokalemia is believed to be due to an intracellular shift of potassium as opposed to total body depletion, as aminoquinolines cause blockade of potassium channels on the pancreatic β-cells [
]. Similar to the mechanism of action of sulfonylureas, hyperinsulinism can produce additional serum abnormalities of hypoglycemia, particularly in patients with underlying metabolic derangements [
]. A variety of neurological effects have been reported, including sensorineural hearing loss, confusion, generalized seizures, dizziness, headaches, hallucinations, CNS depression, and ataxia. Rarely, extrapyramidal effects can be observed and include trismus, coarse tremors, and involuntary movements [
]. Pulmonary edema has also been observed following acute intoxication and is believed to be due to the negative inotropic effects of aminoquinolines [
]. Although severe respiratory depression is rare, the combination of altered mentation, nausea, and vomiting presents significant aspiration risk.
3.2.8 Ototoxicity
While aminoquinolines are less likely than quinine to cause the cinchonism toxidrome consisting of headache, tinnitus, and sensorineural hearing loss, both single doses and chronic use can produce ototoxicity [
]. Hearing loss is typically bilateral, mild to moderate, and may be accompanied by vestibular dysfunction including dizziness and vertigo. In chronic use, these adverse events have been shown to be reversible in some cases with drug cessation. In acute overdose, ototoxicity often resolves within 48 to 72 h [
]. Toxicity occurs via a multifactorial mechanism involving oxidative stress, ischemic damage, and potassium channel inhibition in outer cochlear hair cells leading to hearing loss and vertigo [
]. Onset of ocular symptoms often follows other clinical presentations, such as arrhythmia or hypotension by several hours. Vision improvement may occur rapidly or have a protracted recovery course of months following exposure [
]. Retinal toxicity has been reported at higher cumulative aminoquinoline doses, most often seen with chronic use. Following cumulative doses of 1000 g, the prevalence of retinal toxicity increases to 1% and is associated with an irreversible loss of vision despite cessation of the drug [
]. In some cases, progression of vision loss is present for up to one year after discontinuation of the offending agent. Vision loss is often bilateral and is characterized as a “bull's-eye” maculopathy and depigmentation of the retinal pigment epithelium (RPE) [
]. This begins in the central visual fields, but with continued exposure leads to atrophy of the RPE and visual acuity loss. The mechanism underlying toxicity to the cells of the retina is believed to be multifactorial, including direct photoreceptor damage via alterations in metabolism and secondary effects due to the binding of aminoquinolines to the melanin cells within the RPE [
As opposed to quinine, aminoquinoline toxicity is less commonly associated with acute onset of GI symptoms such as nausea, vomiting, and diarrhea. While these may occur in both acute toxicity and in chronic therapeutic use, there are no long-term GI sequelae [
]. Case reports of drug induced liver injury (DILI) have reported AST and ALT elevations of 399 IU/L and 285 IU/L, respectively, within eight hours of initial dosing [
The devil’s in the dosing: severe drug-induced liver injury in a hydroxychloroquine-naive patient with subacute cutaneous lupus erythematosus and porphyria cutanea tarda.
]. However, in patients with underlying liver disease or porphyria cutanea tarda, DILI has been reported in up to 50% of cases, and observed transaminitis may be much more severe [
The devil’s in the dosing: severe drug-induced liver injury in a hydroxychloroquine-naive patient with subacute cutaneous lupus erythematosus and porphyria cutanea tarda.
Similar to the mechanism underlying aminoquinoline-induced cardiomyopathy, lysosomal dysfunction with vacuolar accumulation of metabolic products is believed to play a role in skeletal muscle toxicity [
]. Clinically, myopathy tends to be mild when symptomatic and affects the proximal muscles to a greater degree than distal groups, presenting as weakness [
The devil’s in the dosing: severe drug-induced liver injury in a hydroxychloroquine-naive patient with subacute cutaneous lupus erythematosus and porphyria cutanea tarda.
]. First, patient underreporting is likely, as elevations in creatine phosphokinase may be seen in patients even with normal strength testing. Second, myopathy may be difficult to distinguish from baseline, as myopathy-related pain and weakness are often associated with the rheumatologic diseases that these drugs are often prescribed to treat [
]. Due to a lack of reduced glutathione, oxidative stress denatures heme, causing extravascular hemolysis. The extent of hemolysis depends on the drug, dose, and the degree of enzyme deficiency, leading to a range of asymptomatic to life-threatening hemolysis [
]. Primaquine is more closely associated with G6PD-mediated hemolysis. Although case report literature describes the finding in chloroquine and hydroxychloroquine use, the largest chart review to date examining these drugs in patients with G6PD noted no occurrence of hemolysis [
Gold-standard evidence such as randomized controlled trials, systematic reviews, or meta-analyses for management of aminoquinoline toxicity do not currently exist in the literature. The following recommendations are based on published expert opinion from poison control centers and medical toxicologists, as well as frequent findings described in case report literature. Consultation with a poison control center and/or medical toxicologist is recommended early in the management of these patients in the emergency department.
Aminoquinoline overdose produces toxicity ranging from mild to severe. Unlike with chloroquine overdoses, there is no established lethal or toxic dose of hydroxychloroquine in adults, and management should be tailored to observed toxicity [
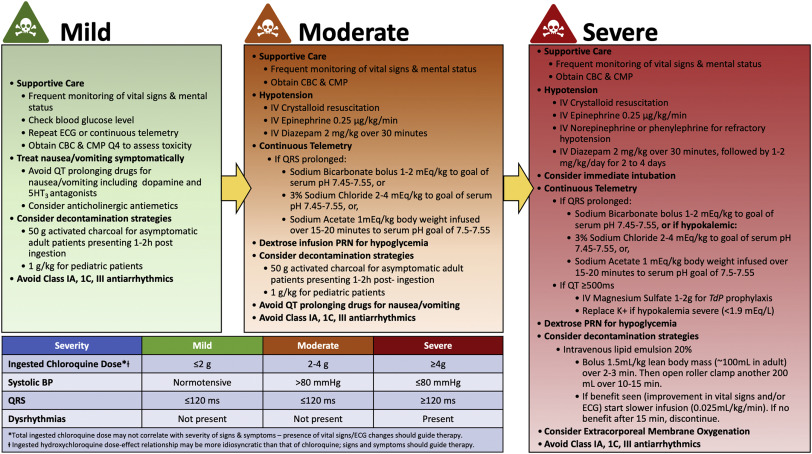
]. Mild chloroquine toxicity in adults is defined as symptomatology occurring with suspected ingested dose <2 g, normal systolic blood pressure, and normal QRS (≤120 ms) [
]. Treatment in the ED setting is focused on high-quality symptomatic and supportive measures, decontamination, stabilization of cardiac dysrhythmias if present, hemodynamic support, and electrolyte correction as necessary [
]. Indications for intensive care unit admission include persistent systemic hypotension, QRS elongation >120 ms, ventricular arrhythmias, seizures, coma, and persistent hypoglycemia [
]. Multiple reports cite early intubation and mechanical ventilation as critical for survival. The combination of altered mentation, apnea, and vomiting present in many aminoquinoline-intoxicated patients heightens the necessity for early and aggressive airway intervention to reduce aspiration risk. Given concerns for rapid potassium shifts in toxicity and repletion, an alternative to succinylcholine should be considered for rapid sequence induction and paralysis to avoid provoking rapid onset of hyperkalemia. Additionally, clinicians should avoid barbiturates for induction, as they may precipitate sudden cardiac arrest [
In the following sections, strategies for the emergency management of aminoquinoline intoxication will be addressed, including decontamination, pharmacotherapeutics, elimination methods, and emerging modalities (i.e. ECMO and ILE). Algorithmic application of these strategies to the categorization of mild, moderate, and severe toxicity is shown in Fig. 1.
Fig. 1Adult algorithmic management of chloroquine and hydroxychloroquine overdose.
Hydroxychloroquine and chloroquine have high volumes of distribution and significant protein binding, complicating modalities for augmenting elimination [
]. Although these drugs are ingested, patients should not receive emetics such as syrup of ipecac, as toxicity sequelae of seizures, altered mentation, dysrhythmias, and hypotension heighten risks of aspiration [
]. Similarly, orogastric lavage has fallen out of favor due to the risks of aspiration. In cases of life threatening ingestion, orogastric lavage can be considered in patients presenting early following ingestion, within one hour [
]. Activated charcoal effectively absorbs aminoquinoline in the gastrointestinal tract with 95%–99% binding when administered in the first five minutes following ingestion [
]. As with other decontamination strategies, the use of activated charcoal will depend on patient presentation (i.e. those who are not nauseated or vomiting) and duration of intoxication [
]. While serum drug levels may be drawn, they are not readily available and therefore are not a practical measure to guide initial management of acute toxicity in the ED setting [
]. However, for inpatient treatment, early and serial measurements of blood chloroquine concentrations are more accurate compared to estimated oral ingestion for predicting cardiovascular severity of chloroquine poisonings [
Blood concentrations are better predictors of chioroquine poisoning severity than plasma concentrations: a prospective study with modeling of the concentration/effect relationships.
Addressing electrolyte abnormalities, dysrhythmias, and blood pressure are the main role of pharmacotherapeutics in the management of aminoquinoline overdose. Hypoglycemia should be managed with dextrose infusion, with careful attention paid to the serum potassium and QT interval. Refractory cases with intractable hypoglycemia (glucose <50 mg/dL) can be managed similar to sulfonylurea toxicity with 50 μg subcutaneous octreotide every 6 h [
]. Hypokalemia is a marker of severity of toxicity in acute poisoning and must be carefully monitored and managed as intracellular shifts can reverse as acute toxicity resolves, with rapid onset of hyperkalemia [
]. Potassium may be repleted cautiously in severe hypokalemia (<1.9 mEq/L), and monitoring of potassium levels should occur regularly. While older studies indicate that hypokalemia may prolong survival, contemporary data favor potassium repletion, generally to >4 mEq/L. [
Prevention of torsade de pointes in hospital settings: a scientific statement from the American Heart Association and the American College of Cardiology Foundation.
]. Epinephrine is the vasopressor of choice in these patients, given the intrinsic negative inotropic effect in aminoquinoline overdose (combination of a α1 and β1 adrenergic receptor blockade) [
]. The literature base supports high-dose epinephrine as the pressor of choice at a starting dose of 0.25 μg/kg/min increased by 0.25 μg/kg/min increments targeting a mean arterial pressure of 65 mmHg [
]. However, epinephrine may exacerbate pre-existing hypokalemia. A study of severely poisoned patients found the addition of high-dose epinephrine to mechanical ventilation increased survival from 9% to 91% [
]. If epinephrine fails to adequately raise mean arterial pressure, a second pressor such as norepinephrine or phenylephrine can be titrated to effect, though alpha agonists increase the effective refractory period and may increase the occurrence of arrythmias [
]. Patients requiring additional vasopressor support beyond epinephrine and diazepam should receive close attention to hemodynamic parameters to ensure treatment efficacy.
Diazepam is used in the management of both hypotension and dysrhythmias in dosages of 2 mg/kg IV over 30 min, followed by 1 to 2 mg/kg/d for 2–4 days in severe cases [
]. The mechanism of diazepam in attenuation of cardiotoxicity is believed to be due to a central antagonistic effect, anticonvulsant effect, antidysrhythmic effect and interaction inverse to aminoquinolines, and decrease aminoquinoline induced-vasodilation [
]. Experimental use of diazepam in animal models of severe chloroquine overdose demonstrates improved systolic and diastolic arterial pressures, heart rate, urine volume, urinary excretion of chloroquine, and shortened QRS duration [
]. No studies have compared efficacy between different benzodiazepines for treatment of acute aminoquinoline toxicity. With medication shortages or variation in ED pharmacy stock, another benzodiazepine may be substituted for treatment of seizures and for maintenance of sedation.
Gastrointestinal symptoms, such as nausea, vomiting, and diarrhea, can be found in mildly intoxicated patients and more severe overdoses. Vomiting in early stages of intoxication may be due to direct irritant effects of aminoquinolines and may be better managed with the decontamination strategies addressed above. Nausea and vomiting can be treated symptomatically while avoiding QTc prolonging agents such as serotonin antagonists (ondansetron) and phenothiazines (promethazine, prochlorperazine) [
]. Antihistamine (meclizine) and dopamine receptor antagonist (metoclopramide) antiemetics may be safer options.
There are currently no accepted treatments for quinine-induced ocular toxicity, but fundoscopic examination, visual field examination, and color testing are appropriate to assess injury ideally by an ophthalmologist [
]. Consideration should be given to the degree of cardiac toxicity and severity of hypokalemia if present, favoring use of sodium acetate or hypertonic saline to avoid worsening hypokalemia. The pH can be used as an indirect indicator of sodium load. When using NaHCO3, a bolus of 1–2 mEq/kg is recommended, repeated as needed to terminate dysrhythmias or narrow QRS complex, followed by a NaHCO3 infusion [
]. Potassium should be closely monitored for intracellular shifting of potassium with development of clinically significant hypokalemia. Hypertonic saline contains the same quantity of sodium in 97 mEq as sodium bicarbonate in 50 mEq. When using 3% NaCl, a bolus of 2–4 mEq/kg may be considered, and sodium levels should be closely monitored [
]. Providers should anticipate the possibility of extended toxicity course in patients with acute and/or chronic renal failure. Unfortunately, hemodialysis use has been reported as ineffective due to high protein binding and large volume of distribution intrinsic to the aminoquinolines [
Blood concentrations are better predictors of chioroquine poisoning severity than plasma concentrations: a prospective study with modeling of the concentration/effect relationships.
]. ECMO may be considered in severe toxicity refractory to standard supportive care and other therapies (i.e. escalation of epinephrine drip rate to >3 mg/h, persistent end-organ failure). One case report describes ECMO initiation on intensive care unit admission following a 9.5 g chloroquine ingestion (initial blood chloroquine concentration 6215 μg/L). The patient presented with altered mental status, left ventricular systolic dysfunction with a dyskinetic interventricular septum, and hypotension unresponsive to crystalloid fluid resuscitation as well as 3 mg/h epinephrine infusion. The patient was weaned from vasopressors on day three, decannulated from ECMO on day four, extubated on day seven, and discharged on day ten with no neurological sequelae [
]. Another case detailing ECMO use in a patient experiencing ventricular fibrillation following 12 g hydroxychloroquine overdose noted “spectacular improvement of hemodynamic parameters and electrocardiographic normalization at day one.” [
]. If benefit is seen in vital signs and/or ECG parameter normalization, slower continuous infusion of ~0.25 mL/kg/min can be administered until resolution of toxicity [
]. Combined ILE, NaHCO3, and vasopressor support has been reported in profound hydroxychloroquine overdose of 40 g presenting with hypokalemia and refractory ventricular fibrillation with positive outcome [
]. Protracted ILE has been associated with dysfunction of ECMO circuits, though this is unlikely in short-term ILE use (<24 h continuous infusion), and case reports have described safe concomitant use of both modalities [
What are the adverse effects associated with the combined use of intravenous lipid emulsion and extracorporeal membrane oxygenation in the poisoned patient?.
Given the wide publicity in the lay media regarding the use of aminoquinolines for COVID-19 and trends in national poison control center data, a more current exploration of the acute management of aminoquinoline toxicity is necessary. This class of drugs has a narrow therapeutic range and a large variance in toxic dose from person to person. Severe symptoms can occur with doses as small as 1.5 g with onset one to three hours post-ingestion. Management of acute toxicity often occurs in the emergency department and should focus on hemodynamic stabilization with the use of early mechanical ventilation, diazepam, epinephrine, frequent ECGs, and repeated blood glucose monitoring, with early step-up to aggressive resuscitative measures including ECMO to support vital functions until the offending agent is metabolized and cleared.
Declaration of Competing Interest
None.
Acknowledgements
All authors conceived the idea for this manuscript and contributed substantially to the writing and editing of the review. This manuscript did not utilize any grants, and it has not been presented in abstract form. This clinical review has not been published, it is not under consideration for publication elsewhere, its publication is approved by all authors and tacitly or explicitly by the responsible authorities where the work was carried out, and that, if accepted, it will not be published elsewhere in the same form, in English or in any other language, including electronically without the written consent of the copyright-holder. This review does not reflect the views or opinions of the U.S. government, Department of Defense, U.S. Army, U.S. Air Force, or SAUSHEC EM Residency Program.
References
Browning D.J.
Pharmacology of chloroquine and hydroxychloroquine.
in: Hydroxychloroquine and chloroquine retinopathy. 2014: 35-63
National Poison Data System (NPDS) Bulletin COVID-19 (Hydroxychloroquine/Chloroquine) [press release]. American Association of Poison Control Centers,
2020
Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention.
Chloroquine diphosphate in two different dosages as adjunctive therapy of hospitalized patients with severe respiratory syndrome in the context of coronavirus (SARS-CoV-2) infection: Preliminary safety results of a randomized, double-blinded, phase IIb clinical trial (CloroCovid-19 Study).
Hydroxychloroquine is much less active than chloroquine against chloroquine-resistant plasmodium falciparum, in agreement with its physicochemical properties.
Therapy and pharmacological properties of hydroxychloroquine and chloroquine in treatment of systemic lupus erythematosus, rheumatoid arthritis and related diseases.
The devil’s in the dosing: severe drug-induced liver injury in a hydroxychloroquine-naive patient with subacute cutaneous lupus erythematosus and porphyria cutanea tarda.
Blood concentrations are better predictors of chioroquine poisoning severity than plasma concentrations: a prospective study with modeling of the concentration/effect relationships.
Prevention of torsade de pointes in hospital settings: a scientific statement from the American Heart Association and the American College of Cardiology Foundation.
What are the adverse effects associated with the combined use of intravenous lipid emulsion and extracorporeal membrane oxygenation in the poisoned patient?.