
Urachal abscess: a cause of adult abdominal pain that cannot be ignored
Correspondence
Urachal abscess: a cause of adult abdominal pain that cannot be ignored
To the Editor:
Omphalitis has once been an important cause of illness and death among neonates throughout the world [1,2]. It is an uncommon disease of the adult. It may be presented with abdominal pain and only mild redness of the surrounding of umbilicus. It cannot be ruled out in adult patients who complain of abdominal pain at emergency department (ED). We report a man with a case of urachal abscess, who presented to our ED with abdominal pain for 1 week.
A 52-year-old man was quite well before. He suffered from periumbilical pain for about 1 week. The character of the pain was not cramping but persistent. Because the pain became more severe, he visited our ED for help. There were no fever, diarrhea, vomiting, and constipation in the recent 1 week. He denied any systemic diseases, major operations, daily medication, or allergic history. On physical examina- tion, blood pressure was 120/80 mm Hg, the body temperature was 36.28C, the heart rate was 76 beats/min, and the respiratory rate was 18 breaths/min. The abdomen was soft, but tenderness and focal rigidity over umbilical area was found. The bowel sound was normoactive. Others were unremarkable.
Laboratory data revealed white blood cell count of 10.48 x 103/lL, hemoglobin level of 14.0 g/dL, and platelet count of 241 x 103/lL. Blood biochemistry was normal. The
standing abdomen x-ray film was normal. He was referred for emergency Abdominal ultrasonography revealing a hypoechoic tract from the umbilicus to abdominal wall (Fig. 1A) and a hypoechoic mass with heteroechogenic content between the peritoneum and the muscle layer (Fig. 1B). The computed tomography (CT) of abdomen arranged later showed focal inflammation with localized abscess formation over the umbilicus, and the surrounding fat planes were infiltrated (Fig. 2). Under the impression of omphalitis with abscess formation, history was traced. According to the patient’s statement, he habitually dug and scratched his umbilicus daily when he took a shower. Discharge from umbilical region was noted 2 to 3 times per year and it usually subsided spontaneously. However, 1 week before admission, he began experiencing abdominal pain. Spontaneous extrusion of the abscess occurred after admission and the pus culture revealed Burkholderia cepacia. He was treated with intravenous amoxicillin/ clavulanate 1.2 g every 8 hours. The abdominal ultrasonog- raphy that followed showed regression of the abscess, and the total resolution occurred on day 26.
Omphalitis, infection of the umbilical cord and/or the surrounding tissues [2], is uncommon in the adult patient and it presented as a slow-paced and milder clinical course than that of newborn [3]. The causes of omphalitis in the adult are not clear, except trauma and abnormalities of the urachus [4]. Greig and Shucksmith [5] excised 6 of 7 cases of omphalitis; they found no sebaceous glands or hair follicles in the umbilical cavity [3]. They found sweat
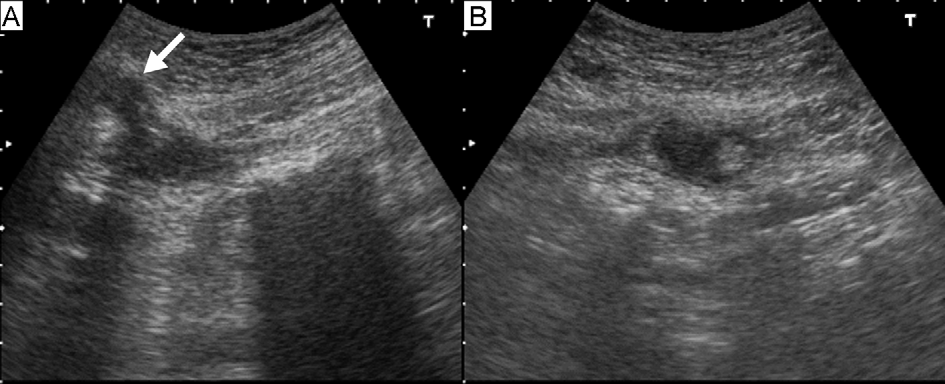
Fig. 1 A, Longitudinal scanning over the umbilicus demonstrated a hypoechoic tract (arrow). B, Transverse scanning over the umbilicus demonstrated hypoechoic mass with heteroechogenic content between the peritoneum and the muscle layer of abdominal wall.
0735-6757/$ - see front matter D 2005 doi:10.1016/j.ajem.2004.03.012

Fig. 2 Abdominal CT showed focal inflammation with local- ized abscess formation over the umbilicus and a tract in the abdominal wall.
glands within the umbilical cavity and the sweat ducts were surrounded by a round cell infiltrate [3]. They proposed that it might progress to dermatitis, stenosis at the skin surface, and abscess formation thereafter [3]. Erythema, edema, and tenderness of the tissues surrounding the umbilicus suggest the diagnosis of omphalitis [6] or urachal abscess. Constant periumbilical pain with or without foul-smelling umbilical discharge may be the initial presentation as our case. Associated signs such as fever, lethargy, and appetite change may implicate systemic complications [6]. Urachal lesions are now better imaged by ultrasonography and CT than by any other image modalities. Demonstration of an abscess within the extraperitoneal fat space of abdominal wall and extension to the umbilicus with or without umbilical discharge is a clue to the diagnosis of urachal abscess [7]. The differential diagnosis of urachal abscess should include hematoma, urachal carcinoma, sarcoma of the abdominal wall [8], peritoneal tumor [9], metastatic carcinoma [10], ventral or umbilical hernia, and inflamma- tory lesions [11]. Omphalitis may be caused by bacteria or fungus [12]. Pus cultures collected by swabs for both aerobic and anaerobic bacteria after proper skin decontam- ination are recommended. If there are obvious systemic signs, blood cultures should also be taken [6]. Although infection of the cord stump is rare, its potential sequelae such as cellulitis, necrotizing fasciitis, peritonitis, multiple hepatic abscess, septicemia, and possible retroperitoneal abscess may be fetal [6,13]. Simple omphalitis, without evidence of periumbilical spread, responds to local applica- tion of antibiotic compresses or ointment [6]. Systemic
antibiotics are indicated if the discharge is purulent or if any evidence of periumbilical spread appears [6].
In summary, omphalitis/urachal abscess may only present as abdominal pain without obvious erythematous perium- bilical tissue or exudates in adults. In spite of rarity in adult patient, it should not be ignored in differential diagnosis of abdominal pain. History taking and detailed physical examination may aid us to early diagnosis at ED. Ultrasonography is a good noninvasive diagnostic tool for suspected cases of urachal lesions and good for following up the response of the medical treatment.
References
- Chamberlain JW. Omphalitis in the newborn. J Pediatr 1936;9: 215 - 22.
- Cushing AH. Omphalitis: a review. Pediatr Infect Dis 1985; 4(3):282 - 5.
- Carny Jr WI, JW, May GA. Omphalitis in the adult. Arch Surg 1973; 106(2):220 - 30.
- Ward TT, Saltzman E, Chiang S. Infected urachal remnants in the adult: case report and review. Clin Infect Dis 1993;16(1):26 - 9.
- Greig GWV, Shucksmith HS. Primary umbilical sepsis in the adult: report of seven cases. Lancet 1950;1:4 - 6.
- Itzhak B. Cutaneous and subcutaneous infections in newborns due to anaerobic bacteria. J Perinat Med 2002;30(3):197 - 208.
- Wan YL, Lee TY, Tsai CC, et al. The role of sonography in the diagnosis and management of urachal abscess. J Clin Ultrasound 1991;19(4):203 - 8.
- Hale JA, Calder IM. Synovial sarcoma of the abdominal wall. Br J Cancer 1970;24:471.
- Yeh HC. Ultrasonography of peritoneal tumors. Radiology 1979; 133:419.
- El-Domeiri A, Whiteley JR. Prognostic significance of abdominal wall involvement in carcinoma of cecum. Cancer 1970;26:552.
- Yeh HC, Rabinowitz JG. Ultrasonography and computed tomography of inflammatory abdominal wall lesions. Radiology 1982;144:859.
- Baruch K. The CO2 laser in omphalitis. J Clin Laser Med Surg 1992;10(2):119 - 21.
- Feo CF, Dessanti A, Franco B, et al. Retroperitoneal abscess and omphalitis in young infants. Acta Paediatr 2003;92(1):122 - 5.
Chia-Chun Hsu MD Yeuh-Ping Liu MD Wan-Ching Lien MD Ting-I Lai MD
Wen-Jone Chen MD Hsiu-Po Wang MD
Department of Emergency Medicine National Taiwan University Hospital
National Taiwan University, College of Medicine
Taipei 100, Taiwan E-mail address: [email protected]