
Sonographic detection of radio-occult interstitial lung involvement in measles pneumonitis
Case Report
Sonographic detection of radio-occult interstitial Lung involvement in measles pneumonitis
Abstract
We present the cases of 23- and 38-year-old healthy patients with clinical diagnosis of acute measles who experienced shortness of breath on exertion with non- productive cough and showed signs of mild respiratory failure at presentation in the emergency department (ED) but with normal chest radiograph and auscultation. In both cases, bedside ultrasound of the lung showed the appearance of signs of interstitial diffuse involvement with vertical B lines spread all over the lateral and posterior chest wall. This sonographic pattern is typical of the interstitial involvement during acute viral pneumonitis that can be missed by physical examination and chest radio- graphy. Even without radiologic infiltrates and pulmonary sounds, based on sonographic and arterial gas signs, a diagnosis of measles pneumonitis was done and patients admitted to the ward for close follow-up and supportive care. We hypothesize a new diagnostic role of bedside lung sonography in screening patients presenting to the ED with initial lung involvement in measles who warrant close follow-up and hospital admission.
Pneumonia is the most common serious complication of measles [1]. Moreover, respiratory failure is the most common cause of death in measles [2]. Adult patients with measles may present to the emergency department (ED) with significant hypoxemia even if they have both normal pulmonary auscultation and chest radiography. Bedside lung ultrasound is a relatively new approach that provides information that is not obtained on chest radiography and has no auscultatory equivalent when using the stethoscope [3]. Detection of the sonographic interstitial syndrome in the ED is useful to the diagnosis of some pulmonary conditions, such as diffuse interstitial pneumonia [4]. This simple sonographic technique relies on the visualization of some echogenic vertical artifacts that originate from the pleural line and spread like laser beams without fading to the edge of the screen. When such artifacts are multiple and displayed bilaterally in more than one thoracic scan, they are a sign of the interstitial syndrome [4].
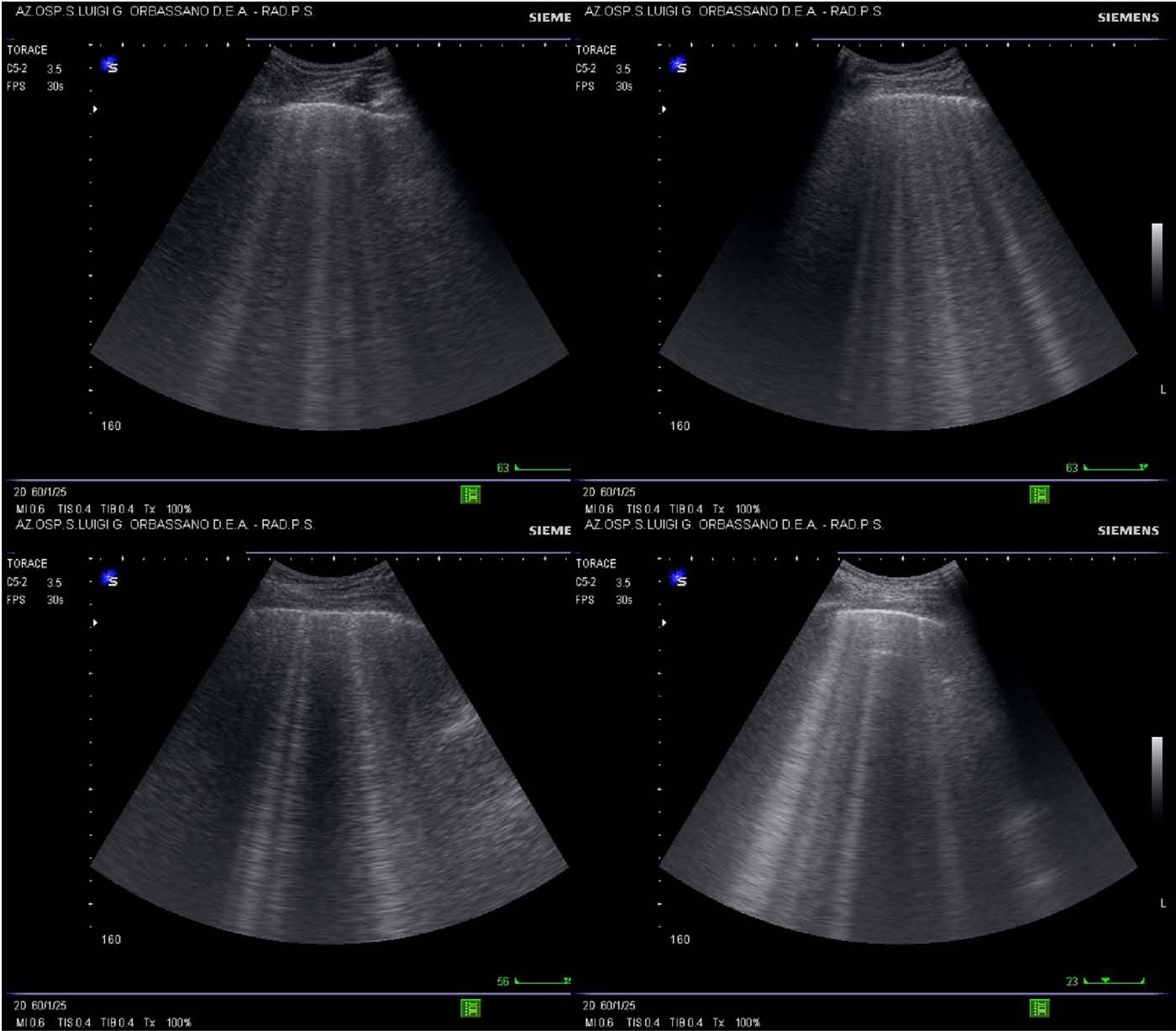
Two patients aged 23 years (male) and 38 years (female) presented to our ED complaining of malaise; high fever with cutaneous brick-red, maculopapular rash; coryza; cough; and conjunctivitis. Diagnosis of primary measles was done because of the typical presentation. They were both unvaccinated healthy patients without history of pulmonary or cardiac diseases. They experienced a mild feeling of shortness of breath on exertion without symptoms and signs of obstructive tracheitis. Respiratory and pulse rates were normal. Chest radiography and auscultation of the thorax wall did not show Pathologic findings (Fig. 1). The male aged 23 years showed a pulse oxymetry saturation of 92% while breathing room air, and the arterial gas analysis revealed a PO2 of 55 mm Hg, PCO2 33.2 mm Hg, pH 7.50. The female aged 38 years showed pulse oxymetry saturation of 94% and PO2 64 mm Hg, PCO2 36 mm Hg, pH 7.44. We performed a bedside lung ultrasound that showed in both cases multiple and bilateral B lines, predominantly visualized in the lateral and dorsal chest scans without pleural consolidations, thus allowing the diagnosis of diffuse interstitial involvement due to measles pneumonitis (Fig. 2). Patients were then admitted to the hospital for a close follow- up and administration of oxygen, antibiotics to prevent bacterial complication, and supportive therapy.
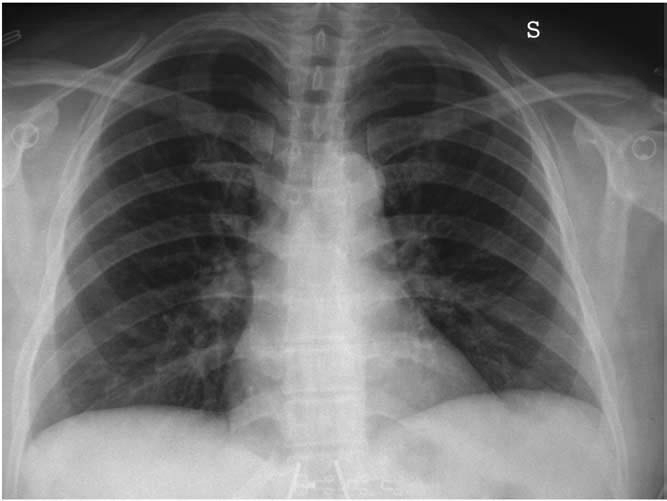
Fig. 1 The case of a 38-year-old healthy patient presenting in the ED with symptoms of measles and mild shortness of breath on exertion. The posteroanterior chest radiograph was normal.
0735-6757/$ - see front matter (C) 2009
 128.e2 Case Report
128.e2 Case Report
Fig. 2 Lung ultrasound pattern in a 38-year-old patient with acute measles and mild respiratory failure. Multiple B lines (vertical echogenic comet tail artifacts) are visualized in the lateral and dorsal scans due to interstitial involvement in measles pneumonitis.
It has been proven that measles can diffusely involve the lung interstitium sufficiently to affect Gas exchange but not sufficiently to result in pulmonary sounds or radiographic findings [5]. This condition usually recovers spontaneously, but sometimes it can progress toward severe respiratory distress and death [6]. For these reasons, it is important to determine the degree of oxygenation in all patients presenting in the ED with symptoms typical of measles even if the routine tests and auscultatory findings are normal. It may be sufficient to initially determine oxygen saturation, but sometimes hyperventilating patients can be misdiag- nosed. In our cases, blood gas determination and lung ultrasound were decisive to detect the lung diffuse interstitial involvement with impairment of gas exchange and to make diagnosis of measles pneumonitis. Typically, the diagnosis of acute pneumonia relies on symptoms of Acute infection that
must be accompanied by the presence of a new radiographic infiltrate or typical auscultatory findings [7]. We know from the literature the flaws of chest radiography in the detection of signs of pneumonia in the ED [8]. From the analysis of our 2 cases, we hypothesize an important role of bedside lung ultrasound in the diagnosis of the pulmonary involvement of patients with primary measles, who deserve close follow-up or hospital admission. These cases show once more that sonography of the lung can be more accurate than radio- graphy in detecting the initial signs of some pulmonary conditions. Sonography has the advantage of being easily implemented in the ED. Moreover, the technique targeted to the detection of the sonographic signs of the interstitial syndrome has a very steep learning curve and can be applied by the same attending emergency physician. This case report introduces a future study on patients with primary measles to
evaluate the true incidence of pulmonary involvement and the usefulness of ED lung ultrasound in the screening of patients with viral pneumonitis.
Giovanni Volpicelli MD Mauro F. Frascisco MD Department of Emergency Medicine San Luigi Gonzaga Hospital
10043 Orbassano, Torino, Italia E-mail address: [email protected]
doi:10.1016/j.ajem.2008.03.052
References
- Dover AS, Escobar JA, Duenas AL, et al. Pneumonia associated with measles. JAMA 1975;234:612-4.
- Beckford AP, Kaschula RO, Stephen C. Factors associated with fatal cases of measles. A retrospective autopsy study. S Afr Med J 1985;68: 858-63.
- Volpicelli G, Frascisco F. Lung ultrasound in the evaluation of patients with pleuritic pain in the emergency department. J Emerg Med 2008;34: 179-86.
- Volpicelli G, Mussa A, Garofalo G, et al. Bedside lung ultrasound in the assessment of alveolar-interstitial syndrome. Am J Emerg Med 2006;24: 689-96.
- Henneman PL, Birnbaumer DM, Cairns CB. Measles pneumonitis. Ann
Emerg Med 1995;26:278-82.
- Swift JD, Barruga MC, Perkin RM, et al. Respiratory failure complicating rubeola. Chest 1993;104:1786-7.
- Niederman MS, Mandell LA, Anzueto A, et al. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med 2001;163:1730-54.
- Campbell SG, Murray DD, Hawass A, et al. Agreement between emergency physician diagnosis and radiologist reports in patients discharged from an emergency department with community-acquired pneumonia. Emerg Radiol 2005;11:242-6.