
Are 2 smaller intravenous catheters as good as 1 larger intravenous catheter?
Brief Report
Are 2 smaller intravenous catheters as good as 1 larger intravenous catheter?
Siu Fai Li MD?, Michael Cole MD, Rhonda Forest MD, Mikaela Chilstrom MD, Eugene Reinersman MD, Michael P. Jones MD, Shreni Zinzuwadia MD, Sheila King MD, Kabir Yadav MS
Department of Emergency Medicine, Jacobi Medical Center, Bronx, NY 10461, USA
Received 25 January 2009; revised 9 April 2009; accepted 3 May 2009
Abstract
Objective: Using Poiseuille’s law and standardized gauge sizes, an 18-gauge (g) intravenous catheter
(IV) should be 2.5 times faster than a 20-g IV, but this is not borne out by observation, in vitro testing, and manufacturer’s data. Our objective was to determine if the infusion rate of a single 18-g IV was equivalent to the infusion rate of two 20-g IVs.
Methods: This was a prospective study in healthy adult volunteers. Subjects simultaneously received 500 mL of normal saline via an 18-g IV in one arm and 500 mL of normal saline via two 20-g IVs in the other arm. We measured the rates of fluid administration. Paired Student’s t test was used for comparison of the 2 arms of the study. We estimated that 18 trials were needed in sample size analysis. Results: Eighteen trials were completed. The mean infusion rate for a single 18-g 500-mL IV administration was 35.6 mL/min (95% confidence interval [CI], 30.3-40.8), with manufacturer’s rating being 105 mL/min. The mean infusion rate for two 20-g IVs was 41.3 mL/min (95% CI, 36.1-46.4), with manufacturer’s rating being 120 mL/min. The rate of infusion via two 20-g IVs were statistically significantly faster than the single 18-g IV, with a mean difference in flow rate of 5.7 mL/min (95% CI, 1.3-10; P = .026).
Conclusion: In healthy volunteers, administration of intravenous fluids through two 20-g IVs is faster than a single 18-g IV, although both approaches are markedly slower than the manufacturer’s estimates.
(C) 2010
Introduction
In emergency medicine, administering intravenous fluids (IVFs) and blood products rapidly may be clinically beneficial in critically ill patients. Advanced trauma and life support guidelines and emergency medicine texts recommend the use of large-bore intravenous catheters
* Corresponding author. Tel.: +1 718 918 5827; fax: +1 718 918 7459.
E-mail address: [email protected] (S.F. Li).
(IVs) in critically ill patients [1,2]. However, variability in patient anatomy, chronic illnesses, and intravenous drug abuse may preclude the placement of a large-bore IV. Simple physics, as stated by Poiseuille’s law, dictates that wider caliber IVs are able to provide higher flow rates, which are a function of the cross-sectional radius raised to the fourth power when other variables such as length and velocity are constant. Calculations based on Poiseuille’s Law using standardized gauge width definitions estimate an 18-gauge
(g) IV to be 2.5 times faster than a 20-g IV in administering maximal flow rates. The implication follows that a single
0735-6757/$ – see front matter (C) 2010 doi:10.1016/j.ajem.2009.05.003
18-g IV should be faster than two 20-g IVs. However, this has not been tested in practice, and in vivo conditions often differ from theoretical calculations.
Past studies in the medical literature have examined IV flow rate variability based on catheter size, tubing type (standard vs large bore), and pneumatic pressure devices, often under in vitro conditions [3-12]. As expected, flow rates were enhanced by larger catheters, larger tubing, and the use of pneumatic devices. We did not find existing clinical data comparing the relative flow rates of a single larger gauge IV and 2 smaller gauge catheters. Manufacturer-supplied data indicate that an 18-g IV is only 1.75 times faster than a 20-g IV (105 vs 60 mL/ min, respectively). However, in day-to-day practice, smaller gauge IVs such as a 20-g IV often seem to provide a flow rate comparable to that of a larger gauge
IV such as an 18-g IV. The observation may not be surprising given that IVs represent only a small, albeit final, portion of the entire intravenous setup, which often includes a much longer segment of tubing in addition to filters and clamps. When we tested an 18-g IV against a 20-g IV by running IVFs using a simple primary tubing setup into a sink, an 18-g IV was only 1.6 times faster than a 20-g IV. Given the conflicting information based on calculations, manufacturer’s data, observation, and in vitro testing, we wished to examine the flow rates of IVs in vivo to estimate intravenous flow rates in human subjects. Our study hypothesis was that there is no difference in the flow rates between a single 18-g IV and two 20-g IVs.
Methods
This was a basic experimental study of healthy volunteers using a matched design. Subjects were recruited by flyers in the emergency department. Volunteers with any medical illnesses, those who were pregnant, and those who did not have adequate venous access (defined as an inability to place two 20-g IVs and one 18-g IV) were excluded from the study. Informed consent was obtained from each subject. The study was approved by our institutional review board.
Subjects had 3 IVs of identical lengths (30 mm) placed into their peripheral veins. A single 18-g IV was inserted in one arm and two 20-g IVs were inserted into separate veins in the contralateral arm. A total of 1000 mL of sterile normal saline was used for the IVF infusion during each trial. Simultaneously, 500 mL of NS was infused through the 18-g IV and 250 mL of NS was infused through each of the two 20-g IVs. All IVs were preferentially placed in the antecubital fossa, and if venous access was not available, IV placement in the forearm and the hand was attempted respectively. All IVs were tested for resistance to flow with saline flushes before IVF infusion. The IVFs were administered through high-flow tubing with the clamp valve “open” via gravity from a single IV pole
raised to maximal height. The time of infusion was measured by stopwatch. The time of infusion of the two 20-g IVs was recorded when the last bag of IVF was completed. The side of the 18-g IV (right vs left) was alternated between volunteers. After each infusion, the volunteer was observed for 30 minutes to ascertain that no adverse reaction had occurred. Volunteers were allowed to undergo consecutive infusions with the same IVs if no adverse reaction was noted.
The primary outcome was the difference in rate of infusion of IVFs through a single 18-g IV compared with two 20-g IVs. Data analysis was performed using simple statistics (means and SDs) and confidence intervals (CIs). Comparison of flow rates between the two modalities was performed using the paired Student t test. We performed in vitro testing by running 500 mL of IVF into a sink with an 18-g IV to estimate our sample size. We estimated that 18 trials were needed to determine a 25 mL/min difference in the flow rates as significant, based on a mean (SD) of 330 (15) seconds from the in vitro testing, a 2-tailed ? of .05, and power of 0.80. Data were analyzed using Stata 9.2 (Stata LP, College Station, TX) and Excel X for Mac (Microsoft, Redmond, WA).
Results
Eighteen trials were completed in 8 volunteers. Two volunteers completed 3 trials of infusions, whereas 6 volunteers completed 2 trials. No volunteer was excluded. There were no adverse effects noted in any of the volunteers. All 18-g IVs were placed in the antecubital fossa. The 20-g IVs were both placed in the antecubital fossa in 2 volunteers, in the antecubital fossa and the forearm in 3 volunteers, and in the antecubital fossa and the hand in 3 volunteers.
intravenous fluid administration via the two 20-g IVs was statistically significantly faster than via the single 18-g IV. The mean flow rate for a single 18-g IV was 35.6 mL/min (95% CI, 30.3-40.8), with manufacturer’s rating being 105 mL/min. The mean flow rate for two 20-g IVs was 41.3 mL/ min (95% CI, 36.1-46.4), with manufacturer’s rating being 120 mL/min (60 mL/min for each of the 20-g IVs). The mean difference in flow rate was 5.7 mL/min (95% CI, 1.3-10; P =
.026), in favor of the two 20-g IVs. The mean time of infusion of 500 mL of IVF via a single 18-g IV was 904 seconds (95% CI, 790-1918), and the mean time of infusion of 500 mL of IVF via two 20-g IVs was 775 seconds (95% CI, 669-881). The mean difference in time of infusion was 129 seconds (95% CI, 17-241).
The difference in flow rates stratified by IV side of the patient (left vs right) was not statistically significant. The mean flow rate of the left-sided IVs was 37.3 mL/min and the mean flow rate of the right-sided IVs was 39.5 mL/min (? = 2.2 mL/min; 95% CI, -6.0-10.0). The IVF ran as
quickly during the first trial as in the second trial (39.2 vs 39.5 mL/min, ? = 0.3 mL/min; 95% CI, -5.5-5.0).
Discussion
In this study of healthy human volunteers, two 20-g IVs provided faster intravenous flow rates than a single 18-g IV did. The comparative flow rates were more consistent with estimations based on in vitro testing and manufacturer’s data than calculations based on Poiseuille’s Law in so far as two 20-g IVs were faster than a single 18-g IV in administering IVFs. However, the actual flow rates were much lower than the flow rates observed in in vitro testing and based on manufacturer’s data. For instance, the mean flow rate of an 18-g IV was only 35.6 mL/min, compared with the flow rate of 105 mL/min provided by the manufacturer. Similarly, the mean flow rate of two 20-g IV was 41.3 mL/min, which was lower than the manufac- turer-labelED flow rate of 60 mL/min for a single 20-g IV. Manufacturer data were similar to the results of our in vitro testing (by running NS into a sink). For instance, the manufacturer label of 105 mL/min of an 18-g IV was comparable to our measured in vitro rate of 91 mL/min.
Our study was not designed for subgroup analysis, but we made several observations during our study. There was no difference between the 2 sides (right vs left) of the IV in terms of flow rates. All of our subjects received multiple infusions, and there was no difference between flow rates in
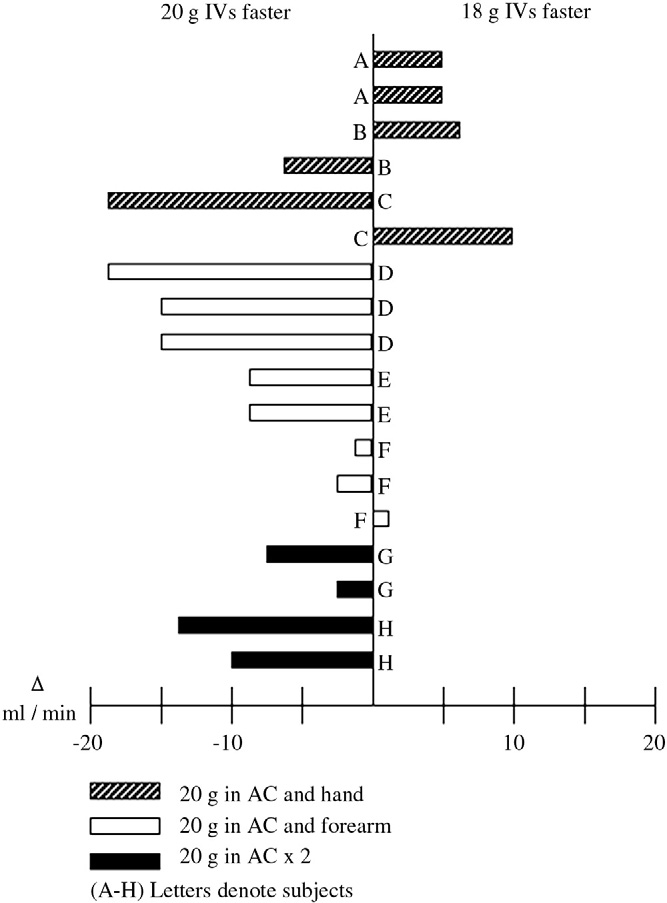
Fig. 1 Comparative flow of single 18-g IV vs two 20-g IVs.
successive trials. The site of the IV (antecubital fossa, forearm, or hand) may have affected our study, as indicated by Fig. 1. There were 5 trials in which the single 18-g IV was faster than the two 20-g IVs. Of the 5 trials, 4 occurred in a subject with a 20-g IV in the hand. It is unclear why the relative flow rates between a single 18-g IV and two 20-g IVs may be altered by the hand IVs. We did not visually detect a significant reduction in flow in the hand IVs when we conducted our trials, and this observation is supported by similar mean flow rates between volunteers who had a 20-g IV in the hand vs volunteers who did not (40.3 vs 41.8 mL/ min, respectively; ? = -1.5; 95% CI, -13 to 9.7). There are several possible explanations for this observation. The negative effect of the hand IVs may be due to peripheral resistance, which inversely affects IVF flow rates [13,14]. Relative flow rates also might be affected because they were placed in series (distal to the antecubital IV) or because of position, smaller caliber veins, remoteness of the IV, or greater variability in flow rates of hand IVs.
During resuscitation, our primary goal is to place the
largest IV possible, as opposed to attempting to place a larger bore IV (>=18 g) in every patient. It is better to have a smaller successful IV that flows smoothly than to “blow” vein after vein in attempts to place a larger bore IV in patients with compromised vascular access. The similar flow rates between two 20-g IVs and a single 18-g IV lend support to this practice.
Limitations
There are several limitations to our study. Our study was conducted in healthy volunteers, and the results may not be generalizable to patients who are volume depleted or in shock. Second, our study does not address the flow rates of other fluids administered through IVs, and given the inherent differences in the viscosity of blood vs NS, our results are unlikely to be generalizable to the administration of blood products. Our study was not designed to detect small differences in potential con- founding variables, such as the side or the site of the IV, and we did not measure other potential confounders such as the pressure of the infusion set-ups or the subject’s blood pressure. It is likely that the site of the IV affected the results of the trial. If we eliminated hand IVs from the study, the two 20-g IVs would be even faster compared with a single 18-g IV. The study may also be biased by the repeated uses of the same IVs in the same subjects, especially in light of the hand effect. Finally, the statistically significant difference in IV flow rates between an 18-g IV and two 20-g IVs may not be clinically significant. A mean difference of approximately 6 mL/min seems unlikely to affect patient outcome. Our study does not address Clinically important outcomes such as efficiency of care, patient satisfaction, and morbidity and mortality.
Conclusion
In healthy volunteers, administration of IVFs through two 20-g IVs is faster than through a single 18-g IV. However, both approaches are markedly slower than flow rates based on calculations, manufacturer’s estimates, or in vitro testing.
References
- Advanced trauma life support: program for doctors, student course manual. 7th ed. Chicago: American College of Surgeons; 2004. p. 77.
- Emergency medicine: a comprehensive study guide, sixth ed. Judith E. Tintinalli, ed. Vascular Access: William Berk, Bharat Sutariya, p.124; Approach to the patient in shock: Emanuel Rivers, Ronny Otero, H. Bryant Nguyen, p. 219. McGraw-Hill, 2004.
- Rottman SJ, Larmon B, Manix T. Rapid volume infusion in prehospital care. Prehosp Disaster Med 1990;5:225-9.
- Iserson KV, Criss E. Combined effect of catheter and tubing size on fluid flow. Am J Emerg Med 1986;4:238-40.
- Iserson KV, Reeter AK, Criss E. Comparison of flow rates for standard and large-bore blood tubing. West J Med 1985;143:183-5.
- Behrendt FF, Bruners P, Keil S. Impact of different vein Catheter sizes for mechanical power injection in CT: in vitro evaluation with use of a circulation phantom. Cardiovasc Intervent Radiol 2009;32:25-31.
- Williamson EE, McKinney JM. Assessing the adequacy of periph- erally inserted central catheters for power injection of intravenous Contrast agents for CT. J Comput Assist Tomogr 2001;25:932-7.
- Mapes A, Jones BR. Enlarging pediatric I.V. catheters. Pediatr Emerg Care 1994;10:18-9.
- Mateer JR, Thompson BM, Tucker J. Effects of high infusion pressure and large-bore tubing on intravenous flow rates. Am J Emerg Med 1985;3:187-9.
- Aedeer MI, Crowe JP, Rhodes RS. Technical limitations in the rapid infusion of intravenous fluids. Ann Emerg Med 1985;14:307-10.
- Dutky PA, Stevens SL, Maull KI. Factors affecting rapid fluid resuscitation with large-bore introducer catheters. J Trauma 1989;29: 856-60.
- Millikan JS, Cain TL, Hansbrough J. Rapid volume replacement for hypovolemic shock: a comparison of techniques and equipment. J Trauma 1984;24:428-31.
- Goodie DB, Philip JH. An analysis of the effect of venous resistance on the performance of gravity-fed intravenous infusion systems. J Clin Monit 1994;10:222-8.
- Elad D. Intravenous infusion: understanding the technical side can improve Clinical performance. J Clin Monit 1994;10:219-21.