
High risk and low prevalence diseases: Open globe injury
a b s t r a c t
Introduction: Open globe injury (OGI) is a rare but Serious condition that carries with it a high rate of morbidity. Objective: This review highlights the pearls and pitfalls of OGI, including presentation, diagnosis, and manage- ment in the emergency department (ED) based on current evidence.
Discussion: OGI refers to full-thickness injury to the layers of the eye. OGI can be caused by blunt or sharp trauma, and subtypes include penetration, perforation, intraocular foreign body (IOFB), globe rupture, or mixed types. OGI is more common in males and usually secondary to work-related injury, but in women it is most commonly associated with falls. Emergency clinicians should first assess for and manage other critical, life-threatening inju- ries. Following this assessment, a thorough eye examination is necessary. Computed tomography (CT) may sug- gest the disease, but it cannot definitively exclude the diagnosis. While Point-of-care ultrasound is highly sensitive and specific for some findings in OGI, its use is controversial due to potential globe content ex- trusion. Management includes protecting the affected eye from further injury, preventing Valsalva maneuvers that could extrude ocular contents, updating tetanus vaccination status, administering broad-spectrum antibi- otics, and ophthalmology consultation for surgical intervention to prevent the sequelae of blindness and endoph- thalmitis.
Conclusion: An understanding of OGI can assist emergency clinicians in diagnosing and managing this sight- threatening traumatic process.
Published by Elsevier Inc.
This article series addresses high risk and low prevalence diseases that are encountered in the emergency department (ED). Much of the primary literature evaluating these conditions is not emergency medicine focused. By their very nature, many of these Disease states and clinical presenta- tions have little useful evidence available to guide the emergency clinician in diagnosis and management. The format of each article defines the dis- ease or clinical presentation to be reviewed, provides an overview of the extent of what we currently understand, and finally discusses pearls and pitfalls using a question and answer format. This article will discuss open globe injury (OGI). This condition’s low prevalence but high morbid- ity, as well as its variable atypical Patient presentations and challenging diagnosis, makes it a high risk and low prevalence disease.
OGI refers to complete penetration of all layers of the eye wall that may lead to endophthalmitis and Vision loss [1]. Subcategories of open
* Corresponding author at: 3551 Roger Brooke Dr, Fort Sam Houston, TX 78234, USA.
E-mail address: [email protected] (B. Long).
globe include laceration versus rupture. Laceration is subcategorized into penetration (only an entry wound present), perforation (entry and exit wounds present), and intraocular foreign body (IOFB). Mixed injury patterns do occur [2,3]. Rupture may occur via blunt trauma, usu- ally at weak points such as the limbus, locations of prior surgery, optic nerve, or rectus muscle insertions on the globe [4-9]. Perforation, pene- tration, and IOFB represent forms of sharp trauma due to lacerations of the globe [2]. Extent of injury can be described using anatomical zones (Fig. 1) [10].
-
- Pathophysiology
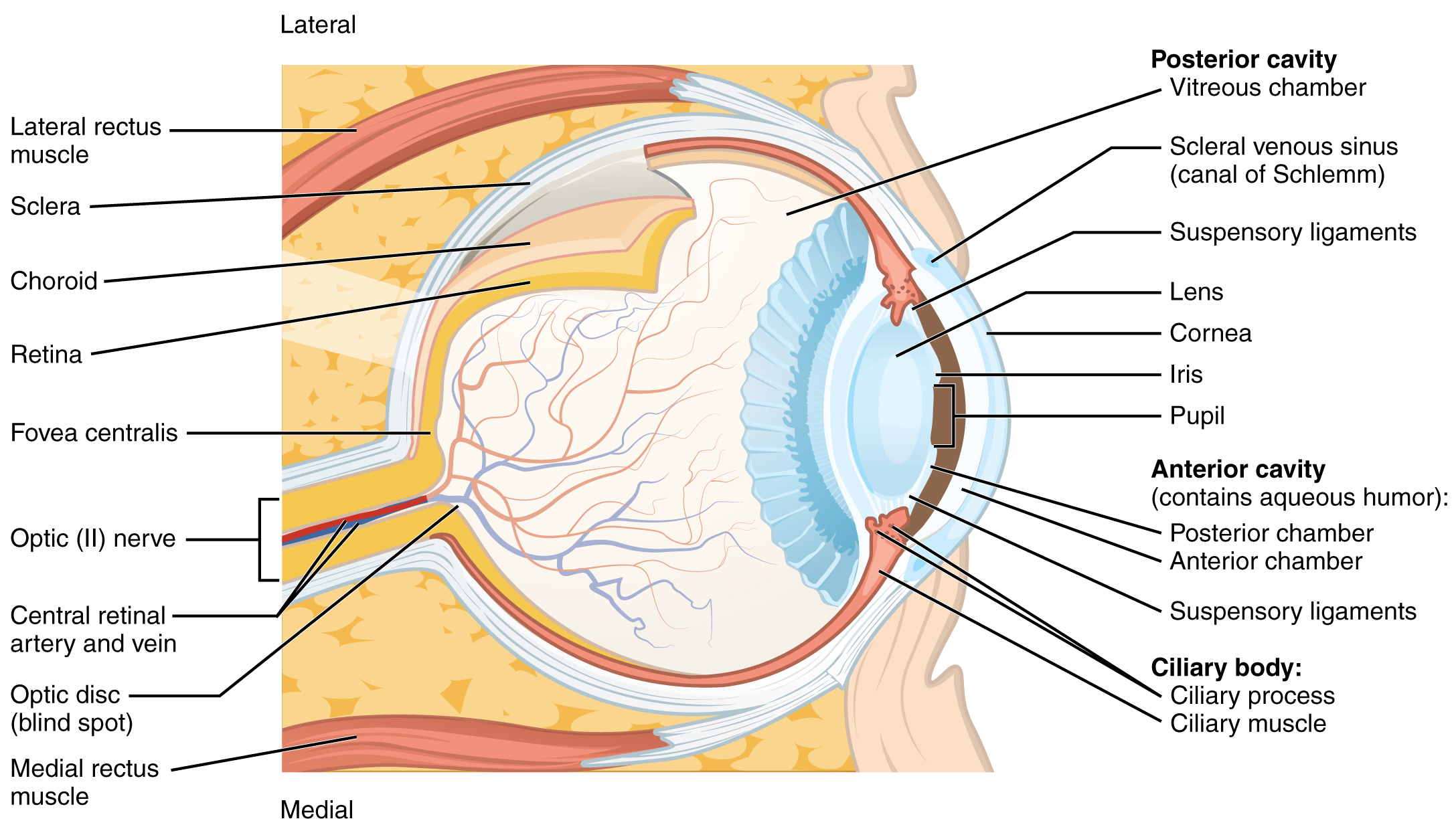
Discussion of the pathophysiology of OGI requires a brief overview of eye anatomy. The eye has three layers, including the cornea (anteri- orly) and sclera (posterior to the limbus); uvea; and the retina. There are three chambers including the anterior chamber, posterior chamber, and vitreous cavity (Fig. 2). The anterior chamber consists of the space between the cornea and anterior edge of the iris/lens and contains Aqueous humor. The posterior chamber extends from the posterior sur- face of the iris to the posterior edge of the ciliary body and the lens and is involved in production and circulation of aqueous humor. The vitreous
https://doi.org/10.1016/j.ajem.2022.11.036 0735-6757/Published by Elsevier Inc.

Fig. 1. Anatomical zones used to describe OGI. Zone 1 extends from cornea to limbus; zone 2 extends from the limbus to 5 mm posterior to the limbus; and Zone 3 involves any area posterior to 5 mm behind the limbus [10]. Image credit: “open globe injuries: Review of Evaluation, Management, and Surgical Pearls” by Zhou et al. Image reproduced with writ- ten permission from Dr. Zhou.
chamber is the largest of the three chambers and extends from the cili- ary body posteriorly to the back of the eye where the retina is located [11]. It contains vitreous humor, which assists in supporting the poste- rior lens and maintaining the ocular shape.
Any traumatic injury may result in OGI. Injuries to the anterior por- tion of the sclera are most common due to scleral thinness anteriorly [12]. In cases of blunt trauma, anterior-posterior force causes the globe to strike against the orbital wall. This increases Intraocular pressure (IOP) and leads to scleral tearing at points of weakness [13]. OGI
associated with Penetrating injuries involves the cornea in the majority of cases, though approximately one-third of injuries will involve the sclera or limbus [14,15]. An IOFB can be present in a globe laceration. IOFB are found in the vitreous cavity most commonly, followed by the anterior chamber, retina, and lens [15]. With any violation of the protec- tive wall of the eye, there is potential for extrusion of intraocular con- tents, especially with increases in IOP [16,17]. There is also a significant risk of endophthalmitis following OGI, with rates ranging be- tween 2 and 8%, though if an IOFB is present, up to 30% of patients with OGI can experience endophthalmitis [15,18-22]. Other factors associ- ated with infection include presenting with decreased visual acuity, globe laceration, injury with organic material (e.g., dirt, plant matter from gardening, etc.), lens disruption, and delayed operative care [15,18-22]. The final complication in those who are not appropriately treated includes complete vision loss [1,23].
-
- Epidemiology
The incidence of OGI is 2-6 cases per 100,000 population [24]. Males account for approximately 80% of cases, with most cases occurring be- tween the ages of 10-30 years [25-28]. This risk of OGI due to a blunt mechanism is increased after ocular surgery, including cataract removal, corneal transplant, and laser-assisted in situ keratomileusis (LASIK) [4,5,29,30]. Osteogenesis imperfecta and Ehlers-Danlos syndrome in- crease the risk of OGI in the setting of eye trauma due to a weakness of the sclera [31-34]. In children, injury is typically associated with eye laceration from a sharp object [27,35,36]. In male adolescents, penetrat- ing injury due to a projectile may result in OGI, as well as motor vehicle accidents, fights, and sports [26,28]. OGI occurring in males is most com- monly due to a penetrating injury experienced at work while not wear- ing protective eyewear [1,37,38]. Illicit drug or alcohol use can be a contributing factor in this population as intoxication may increase the risk for traumatic injury [28,39]. In elderly patients, globe rupture is more common compared to globe laceration, with a fall being the most common mechanism [1,25,37,38,40]. IOFB account for 18-41% of
Fig. 2. Anatomy of the eye. Open-access image obtained from: https://upload.wikimedia.org/wikipedia/commons/1/15/1413_Structure_of_the_Eye.jpg.
{kind=link}
OGI, which are most commonly small projectiles [41-43]. Several factors are associated with OGI, including low socioeconomic status , likely because this sector of the population tends to work more danger- ous jobs [40]. Failure to use protective eyewear increases OGI risk, espe- cially in construction settings [44].
- Discussion
- Presentation
OGI should be suspected in any case of blunt or penetrating injury to the eye. History including the time and mechanism of injury is integral to obtain, as well as suspicion of an IOFB and prior ocular procedures. Patients will present with eye pain and typically decreased visual acuity [45]. Emergency clinicians should be suspicious for OGI if there are inju- ries to the adnexa (such as lacerations), orbital floor fracture, or retrobulbar hemorrhage, as approximately 25% of OGI patients have in- juries to the orbit or adnexa (e.g., the eyelids, lacrimal gland and duct, and all other contents of the orbit with the exception of the globe and optic nerve) [46,47].
-
- ED evaluation
Emergency clinicians should first assess for and manage other criti- cal, life-threatening injuries. Following this assessment, patients with suspected OGI should undergo a full eye examination, including visual acuity, pupils including Afferent pupillary defect (APD), confrontational visual fields, Extraocular movements, gross examination with slit lamp or pen light, and fluorescein staining. Potential physical examination findings in OGI include decreased visual acuity, pupillary shape abnor- malities such as a teardrop or peaked pupil (Fig. 3), an APD, abnormal extraocular movements (if there is an associated orbital floor fracture with extraocular muscle entrapment syndrome), corneal or scleral de- fects, and positive Seidel test (a rivulet of fluorescein flowing from a cor- neal or scleral defect in OGI) (Fig. 4) [14,48]. It is critical to note that assessment of IOP should be avoided as part of the Ocular examination
Fig. 3. Peaked pupil from open globe. Obtained from https://webeye.ophth.uiowa.edu/ eyeforum/atlas/pages/peaked-pupil-from-open-globe.html. Ophthalmic Atlas Images by EyeRounds.org, The University of Iowa are licensed under a Creative Commons Attribu- tion-NonCommercial-NoDerivs 3.0 Unported License.
Fig. 4. Corneal perforation, positive Seidel test. Obtained from https://eyerounds.org/atlas/ pages/corneal-perforation-seidel-posative-.html. Ophthalmic Atlas Images by EyeRounds. org, The University of Iowa are licensed under a Creative Commons Attribution-NonCom- mercial-NoDerivs 3.0 Unported License.
in patients with suspected OGI, as placing pressure on the eye may the- oretically cause extrusion of orbital contents [48]. Imaging using com- puted tomography (CT) of the eye with thin cuts without contrast can also be used in the evaluation for OGI. Ultrasonography is another imaging modality, but any pressure placed on the globe could theoreti- cally lead to orbital content extrusion [49]. If US is performed, copious amounts of gel should be applied in order to avoid placing pressure on the globe [49]. Neither imaging modality can definitively rule out the disease, and thus ophthalmology consultation should not be delayed to obtain imaging if there is High clinical suspicion for this diagnosis.
-
- ED management
Management focuses on preventing further ocular injury, avoiding increases in IOP, administering antibiotics, and emergent ophthalmol- ogy consultation. Penetrating foreign bodies should not be removed, as this could lead to extrusion of vitreous from the eye and exposure to further environmental pathogens, raising the risk for endophthalmi- tis. Efforts should be made to decrease IOP by elevating the head of the bed and treating anxiety, nausea, and pain. Any Valsalva maneuver should be avoided, as this could lead to extrusion of eye contents [48]. Tetanus vaccination status should be updated [50]. Broad-spectrum in- travenous antibiotics that penetrate the globe should be administered, such as ciprofloxacin, levofloxacin, moxifloxacin, or ceftazidime with vancomycin [51-55]. Antifungal agents may be required in select cases (e.g., OGI involving dirt or IOFB) after consultation with the ophthalmol- ogy specialist. Topical antibiotics such as moxifloxacin may also be ad- ministered, but this should be discussed with the ophthalmology specialist [14]. Definitive management is surgical, and emergent oph- thalmology consultation is recommended.
- Pearls and pitfalls
- What is the systematic approach to the patient with painful versus painless monocular vision loss?
The optic chiasm represents a dividing point for vision loss. Pathol- ogy anterior to the chiasm causes monocular vision loss, and pathology
posterior to the chiasm causes binocular vision loss [56]. Monocular vi- sion loss can be due to pathology of the globe or the optic nerve. Positive symptoms (i.e., additions to vision, also known as photopsias) including wavy images, warped images, and flashing lights suggest retinal (globe) pathology [57,58]. Optic nerve damage can cause faded color vision. The presence of an APD suggests damage to the optic nerve, and absence of an APD (or normal pupillary reaction to light) is more suggestive of oc- ular pathology [57]. Central or retinal pathology leads to negative symp- toms (i.e., complete or incomplete vision loss) rather than positive symptoms [58].
The clinician should next determine the time course of the monocu- lar vision loss. For example, if the progression has been chronic (months to years), pathology such as macular degeneration or cataracts is more likely [56]. Subacute (days to weeks) development of vision loss could be associated with diseases such as Optic neuritis [56]. Acute onset (sec- onds to minutes) may be associated with rapidly-developing processes such as OGI, retinal or vitreous detachment, or acute angle closure glau- coma. Transient Visual loss can also occur, such as in cases of amaurosis fugax [56].
These factors will significantly narrow the differential diagnosis to whether the cause of the vision loss is ocular or due to optic nerve pa- thology. Several other considerations can further narrow the differential diagnosis (Fig. 5). If there are associated focal neurologic deficits, central pathology such as ischemic stroke, Transient ischemic attack , or Multiple sclerosis should be suspected [58,59]. Vascular risk factors should raise suspicion for Central retinal artery occlusion (CRAO), central retinal vein occlusion (CRVO), or TIA [60]. If the patient has been exposed to medications or toxins in the anticholinergic or sympathomimetic classes, acute angle closure glaucoma should be considered [56].
-
- What are high-yield features of the history for OGI?
Several historical factors are suggestive of OGI. A retrospective, cross-sectional study of ED patients found the most common mecha- nisms of OGI from highest to lowest frequency included striking against
an object or person (32.1%), cutting or piercing (15.1%), accidental entry of a foreign body (14.6%), fall (9.6%), assault (8.2%), motor vehicle colli- sion (2.9%), firearms (1.4%), and machinery (1.0%) [40]. A five-year ret- rospective case series involving 205 OGI at a tertiary care hospital found the most common mechanism of injury causing penetration or IOFB was working with metal [68]. For IOFB, other mechanisms of injury included gardening and construction [68]. For penetrating injuries, the most common mechanisms after working with metal are assault, construc- tion, working with glass or porcelain, wood chopping, gardening, being pecked by a bird, broken kitchen items or glass, or being stabbed with a writing implement [68]. Another five-year retrospective cohort study including 104 patients found work-related accidents were the most common mechanism causing OGI, followed by falls, in-home acci- dents, assaults, hunting accidents, and sport or traffic accidents [1].
While the level of detail collected regarding mechanism of injury
varies between each of the aforementioned studies, and there is some variation in the causes of OGI geographically, work-related injuries seem to universally be the most common cause of OGI. Patients present- ing with eye pain or vision changes after a work-related accident or one of the traumatic mechanisms previously mentioned should raise con- cern for OGI.
-
- What findings on examination suggest OGI?
A comprehensive ocular examination is necessary after evaluating for other life-threatening injuries. Visual acuity should first be assessed starting with a Snellen chart. If a patient is unable to see the Snellen chart, the emergency clinician should evaluate for ability to count fin- gers, followed by detection of hand motion and then light perception.
When examining the pupils, the emergency clinician should exam- ine for abnormal contour or a relative APD. An APD may or may not be present in OGI. If an APD is present in the setting of OGI, it suggests con- comitant injury to the optic nerve and a worse prognosis [69].
As with all eye examinations, the clinician should assess confronta- tional visual fields and extraocular movements. OGI can be associated
Fig. 5. Approach to monocular vision loss [61-67].
with orbital floor fractures and subsequent orbital muscle entrapment, leading to abnormal extraocular movements [14,70].
Gross examination should be performed using a penlight or slit lamp. Penetrating or perforating injuries can be subtle, and evidence of uveal prolapse may be present. Globe rupture is typically more obvi- ous, with extruded orbital contents such as vitreous, iris, or lens. The classic presentation involves a teardrop-shaped or peaked pupil, which points toward the site of injury (Fig. 3). Hyphema or 360 degree subconjunctival hemorrhage can be associated with OGI [14]. Slit lamp examination may demonstrate a shallow anterior chamber in anterior OGI and deep anterior chamber in posterior OGI [45,48].
If the physical examination is not diagnostic of OGI up to this point, the clinician should assess for a positive Seidel test. To perform this test, the clinician applies Topical anesthetic eye drop to the affected eye, followed by application of a moistened fluorescein strip to the area with the suspected leak. Clinicians may also apply the fluorescein to the superior conjunctiva, allowing the dye to flow down the cornea. The clinician then uses either a Woods lamp or cobalt blue light to eval- uate for visible fluorescein flow, which is diagnostic of OGI (Fig. 4) [51]. This test is unnecessary if there is obvious globe rupture.
Literature suggests that emergency clinicians should not evaluate ocular pressure in cases of suspected OGI, since this may lead to orbital content extrusion [14]. However, there are no case reports or peer re- viewed data documenting extrusion of ocular contents from ocular pressure evaluation in the ED setting. If an OGI is not initially suspected and ocular pressure is evaluated, it will most likely be low (less than 10 mmHg), which should raise concern for a scleral injury [72].
-
- What is the utility of CT for diagnosis?
Imaging may be used in assessment for OGI, including CT of the eye without contrast using 1-2 mm cuts. CT findings suggestive of OGI in- clude IOFB (only reliable for radiopaque objects), intraocular air, volume loss in the eye, decreased depth of the anterior chamber, globe defor- mity, displaced lens, and irregular scleral contour (Figs. 6 and 7) [73-78]. CT is more reliable than other imaging modalities for the iden- tification of IOFB and has the additional benefit of ruling out concomi- tant orbital floor fracture which is concerning for OGI [79,80].
A retrospective study of 75 Ocular trauma patients with 76 injured globes found the sensitivity and specificity of CT were 76% and 85%, respectively, for OGI [70]. Another retrospective study found the sensi- tivity and specificity of CT were 51-77% and 97%, respectively [73]. A third retrospective study of 200 patients presenting from 1989 to 1993 found the sensitivity and specificity of CT to be 75% and 93% [81], while a retrospective study of 46 patients found the sensitivity and specificity of CT were 56-68% and 79-100%, respectively [82]. Based on the data, overall CT sensitivity ranges from 51 to 77% and spec- ificity from 79 to 100% [51,70,73,81,82]. Given the limited sensitivity of CT for identifying OGI, this modality should not be used in isolation to rule out OGI, though several findings may suggest the diagnosis.
The use of US for the diagnosis of OGI is controversial. The sensitivity of emergency clinician performed point-of-care US (POCUS) in evalua- tion for OGI may be higher than CT. A prospective cohort study of 232 patients found the sensitivity and specificity of POCUS for globe rupture was 100% and 99.7%, respectively [83]. The emergency clinicians per- forming the POCUS completed 16 h of didactic training and 48 h of hands-on scanning time with ocular POCUS prior to the study, which is likely far more training than most emergency clinicians have in Ocular US. This study only included four patients with true positive globe rup- ture, so it is difficult to draw definitive conclusions [83]. In a prospective observational study conducted in a suburban community hospital affil- iated with a residency program in the U.S., 61 ocular trauma patients were enrolled, and three were found to have penetrating ocular injuries.
Fig. 6. CT demonstrating reduced size and irregular shape of the right globe, with posteri- orly subluxated lens, consistent with OGI. Case courtesy of Assoc Prof Frank Gaillard, Radiopaedia.org, rID: 5348.
POCUS was performed by attending and resident emergency physicians. The attendings received no specific ocular POCUS training prior to the study but had all performed more than 15 prior ocular US examinations, and the residents received one hour of didactics and one hour of hands- on time from the attendings prior to the study. Specificity was 97.2% and sensitivity was 100% for ocular pathology (including CRAO, CRVO, IOFB, lens dislocation, OGI, retinal detachment, retrobulbar hematoma, or
Fig. 7. CT demonstrating reduced size of the globe, reduced anterior chamber depth, and IOFB, consistent with OGI. Case courtesy of Dr. Dalia Ibrahim, Radiopaedia.org, rID: 28527.
vitreous detachment or hemorrhage) of the entire cohort when com- paring POCUS to thin-slice CT and/or ophthalmology evaluation in the ED. Unfortunately, the sensitivities and specificities of POCUS for OGI were not separately calculated [84]. In a porcine model, emergency medicine residents (post-graduate years I-III) had an average accuracy of 89% in the detection of IOFB using POCUS. Accuracy increased by year of training, suggesting that more experience enhances degree of accuracy with the use of POCUS for detecting IOFB [85].
The concern with POCUS is that any pressure placed on the eye could lead to extrusion of intraocular contents. Most studies evaluating the use of POCUS for posterior globe injuries exclude patients with OGI. The prospective studies and case reports that have evaluated the use of POCUS for globe rupture did not demonstrate any adverse events, but further data are required before this is utilized routinely for diagno- sis given the small numbers of patients involved [74,75,83,84,86]. If emergency clinicians perform POCUS to assess for OGI when physical examination findings alone are insufficient, they must use copious amounts of ultrasound gel and rest the hand firmly on the bridge of the nose to avoid placing any direct pressure on the eye [49].
-
- What are the key evidence-based components of management?
Early and aggressive surgical intervention is the most important component of management for OGI. Intervention within 12-24 h is as- sociated with lower rates of endophthalmitis and improved vision [87,88]. While outcomes can be poor if surgical intervention is delayed, up to 54% of appropriately treated patients can have sufficient vision to be measurable with a Snellen chart after OGI [88]. Among all patients with OGI, approximately 9% of people ultimately have no light percep- tion, and 39% experience 20/40 vision or better in the affected eye [89].
The key components of ED management for OGI include:
- Early ophthalmology consultation [14].
- Placing an eye shield over the eye to protect it from further damage.
- Avoiding removal of foreign bodies [48].
- Making the patient nil per os (NPO).
- Treating pain and nausea to prevent Valsalva maneuver that could be associated with crying or vomiting [14].
- Updating tetanus vaccination status if needed [50].
- Administering broad-spectrum antibiotics, including vancomycin and a third- or fourth-generation cephalosporin (which can be substituted with a quinolone if the patient has a cephalosporin al- lergy). Antifungal coverage should be added in discussion with the ophthalmologist if the OGI involves dirt or there is an IOFB [55,90]. Ophthalmology may proceed with intravitreal injection of ampho- tericin B or voriconazole given the lower risk of systemic side effects [91-93]. Oral and intravitreal fluconazole have also been used for OGI; oral fluconazole has fewer systemic side effects than the afore- mentioned agents and good penetration of the eye [54,94-96].
A variety of factors are associated with prognosis and visual out- comes, though as discussed, presenting visual acuity after the injury and time to operative intervention are the most important [87,88]. Se- verity and mechanism of the initial injury, and the initial examination findings, are important prognostic factors in visual outcomes as well [87,88]. Blunt mechanism of injury, initial visual acuity of hand move- ments or worse, relative afferent pupillary defect, posterior wound loca- tion, metallic IOFB, Associated injuries (e.g., lid laceration, lens damage, hyphema, retinal detachment, vitreous hemorrhage), and endophthal- mitis are associated with poor prognosis [4,11,21,81,82,97-99]. The Oc- ular Trauma Score (OTS) is a point system utilized for prognosis based on several factors, including initial visual acuity, globe rupture, endoph- thalmitis, perforating injury, retinal detachment, and APD [100]. Raw
Table 1
Open globe injury pearls.
-
-
- OGI occurs with complete penetration of all layers of the eye wall that may lead to endophthalmitis and vision loss.
- The extent of injury in OGI can be described using anatomical zones.
- Visual prognosis is determined by several factors, including the Ocular Trauma Score and time to surgical intervention.
- High-velocity projectiles or direct blunt trauma to the globe should raise con- cern for OGI, especially if there are associated Facial fractures or injuries to the adnexa.
- The classic patient with OGI is a male injured at work, but the disease must be considered in any traumatic mechanism, including elderly patients with falls.
- Suspected OGI patients should undergo a thorough ophthalmologic examina- tion; however, assessment of ocular pressure is not recommended in the ED.
- Classic examination findings include a peaked or teardrop pupil and positive Seidel test.
- OGI is a clinical diagnosis; imaging with CT may suggest the disease, but it cannot definitively exclude it.
- POCUS is controversial and should likely be avoided at the current time.
- Treatment includes covering the eye with an eye shield, avoiding removal of any foreign bodies, preventing Valsalva maneuvers, ensuring adequate tetanus vac- cination status, and administering broad-spectrum antibiotics. Fungal coverage should be considered for those with soil involvement or cases of IOFB.
- Emergent consultation with ophthalmology is recommended, as visual progno- sis is worse if operative intervention is delayed over 24 h.
-
scores calculated from zero to 100 based on these factors are then com- puted into an OTS ranging from one to five, with higher scores correlat- ing with better visual prognosis [100]. A separate model utilizes initial visual acuity, lid laceration, relative afferent pupillary defect, and poste- rior wound location, which has a sensitivity of 86% and specificity of 92% for predicting survival of vision [23]. Elderly patients and patients less than five years old also have worse Visual outcomes [1,101].
Table 1 provides pearls concerning the evaluation and management
of OGI.
- Conclusion
OGI is a full-thickness traumatic injury to the wall of the eye (cornea or sclera) associated with severe morbidity. Injury can be caused by blunt or penetrating mechanisms, and subtypes include penetration, perforation, IOFB, or globe rupture. If untreated, patients can experience endophthalmitis and vision loss. Poor visual acuity after the injury, globe rupture, IOFB, older women, children, and delays in surgical inter- vention are associated with worse prognosis. OGI is a clinical diagnosis, classically presenting with painful visual loss, pupillary shape abnor- malities (with the pupil “pointing” to the site of injury), and positive Seidel test. CT may be helpful for confirming the diagnosis of OGI, but it cannot definitively rule out the disease. POCUS has high sensitivity and specificity for several findings in OGI, but its use is controversial at this time. Management focuses on protecting the globe from extrusion of orbital contents via a protective shield and avoidance of Valsalva ma- neuvers, updating tetanus vaccination status, broad-spectrum antibi- otics, and early surgical intervention by ophthalmology. Early diagnosis and management are key to ensuring the best possible visual outcomes for the patient.
CRediT authorship contribution statement Jessica Pelletier: Writing - review & editing, Writing - original draft,
Visualization, Conceptualization. Alex Koyfman: Writing - review &
editing, Visualization, Validation, Supervision. Brit Long: Writing - review & editing, Writing - original draft, Visualization, Validation, Supervision.
Declaration of Competing Interest
None.
JP, BL, and AK conceived the idea for this manuscript and contributed substantially to the writing and editing of the review. This manuscript did not utilize any grants, and it has not been presented in abstract form. This clinical review has not been published, it is not under consideration for publication elsewhere, its publication is approved by all authors and tacitly or explicitly by the responsible authorities where the work was carried out, and that, if accepted, it will not be published elsewhere in the same form, in English or in any other language, including electroni- cally without the written consent of the copyright-holder. This review does not reflect the views or opinions of the U.S. government, Depart- ment of Defense, U.S. Army, U.S. Air Force, or SAUSHEC EM Residency Program.
References
- Guzman-Almagro E, Fernandez-Sanz G, Herrero-Escudero D, Contreras I, Gonzalez Martin-Moro J. Open-globe-injury: a single center Spanish retrospective 5-year co- hort study. Eur J Ophthalmol. 2021;31(5):2710-6. https://doi.org/10.1177/ 1120672120962039.
- Kuhn F, Morris R, Witherspoon CD, Heimann K, Jeffers JB, Treister G. A standardized classification of ocular trauma. Ophthalmology. 1996;103(2):240-3. https://doi. org/10.1016/S0161-6420(96)30710-0.
- Al-Omran AM, Abboud EB, Abu El-Asrar AM. Microbiologic spectrum and visual outcome of posttraumatic endophthalmitis. Retina Phila Pa. 2007;27(2):236-42. https://doi.org/10.1097/01.iae.0000225072.68265.ee.
- Zeiter JH, Shin DH. Traumatic rupture of the globe after glaucoma surgery. Am J Ophthalmol. 1990;109(6):732-3. https://doi.org/10.1016/s0002-9394(14)72447- x.
- Lambrou FH, Kozarsky A. Wound dehiscence following cataract surgery. Ophthal- mic Surg. 1987;18(10):738-40.
- Olsen TW, Aaberg SY, Geroski DH, Edelhauser HF. Human sclera: thickness and sur- face area. Am J Ophthalmol. 1998;125(2):237-41. https://doi.org/10.1016/S0002- 9394(99)80096-8.
- Cherry PMH. Rupture of the globe. Arch Ophthalmol. 1972;88(5):498-507. https:// doi.org/10.1001/archopht.1972.01000030500006.
- Cherry PMH. Indirect traumatic rupture of the globe. Arch Ophthalmol. 1978;96
(2):252-6. https://doi.org/10.1001/archopht.1978.03910050120003.
- Riffenburgh RS. Contusion rupture of the sclera. Arch Ophthalmol. 1963;69(6): 722-6. https://doi.org/10.1001/archopht.1963.00960040728007.
- Pieramici DJ, Sternberg P, Aaberg TM, et al. A system for classifying mechanical in- juries of the eye (globe). Am J Ophthalmol. 1997;123(6):820-31. https://doi.org/ 10.1016/S0002-9394(14)71132-8.
- Grant-Kels JM, Kels BD. Human ocular anatomy. Dermatol Clin. 1992;10(3): 473-82. https://doi.org/10.1016/S0733-8635(18)30316-4.
- Vurgese S, Panda-Jonas S, Jonas JB. Scleral thickness in human eyes. PLoS One. 2012;7(1):e29692. https://doi.org/10.1371/journal.pone.0029692.
- Kumar K, Figurasin R, Kumar S, Waseem M. An uncommon meridional globe rup- ture due to blunt eye trauma. Case Rep Emerg Med. 2018;2018:1808509. https:// doi.org/10.1155/2018/1808509.
- Zhou Y, DiSclafani M, Jeang L, Shah AA. Open globe injuries: review of evaluation, management, and surgical pearls. Clin Ophthalmol. 2022;16:2545-59. https://doi. org/10.2147/OPTH.S372011.
- Williams DF, Mieler WF, Abrams GW, Lewis H. Results and prognostic factors in penetrating ocular injuries with retained intraocular foreign bodies. Ophthalmol- ogy. 1988;95(7):911-6. https://doi.org/10.1016/s0161-6420(88)33069-1.
- Navon SE. Management of the ruptured globe. Int Ophthalmol Clin. 1995;35(1): 71-91. https://doi.org/10.1097/00004397-199503510-00009.
- Pelayes Kuhn Fand, DE. Management of the ruptured eye. Eur Ophthalmic Rev. 2009;03(01):48. https://doi.org/10.17925/EOR.2009.03.01.48.
- Duch-Samper AM, Menezo JL, Hurtado-Sarrio M. Endophthalmitis following pene- trating eye injuries. Acta Ophthalmol Scand. 1997;75(1):104-6. https://doi.org/10. 1111/j.1600-0420.1997.tb00263.x.
- Thompson JT, Parver LM, Enger CL, Mieler WF, Liggett PE. Infectious endophthalmi- tis after penetrating injuries with retained intraocular foreign bodies. National eye Trauma system. Ophthalmology. 1993;100(10):1468-74. https://doi.org/10.1016/ s0161-6420(93)31454-5.
- Thompson WS, Rubsamen PE, Flynn HW, Schiffman J, Cousins SW. Endophthalmitis after penetrating trauma. Risk factors and visual acuity outcomes. Ophthalmology. 1995;102(11):1696-701. https://doi.org/10.1016/s0161-6420(95)30807-x.
- Verbraeken H, Rysselaere M. Post-traumatic endophthalmitis. Eur J Ophthalmol. 1994;4(1):1-5. https://doi.org/10.1177/112067219400400101.
- Boldt HC, Pulido JS, Blodi CF, Folk JC, Weingeist TA. Rural endophthalmitis. Ophthal-
mology. 1989;96(12):1722-6. https://doi.org/10.1016/s0161-6420(89)32658-3.
- Schmidt GW, Broman AT, Hindman HB, Grant MP. Vision survival after open globe injury predicted by classification and regression tree analysis. Ophthalmology. 2008;115(1):202-9. https://doi.org/10.1016/j.ophtha.2007.04.008.
- Knyazer B, Levy J, Rosen S, Belfair N, Klemperer I, Lifshitz T. Prognostic factors in posterior open globe injuries (zone-III injuries). Clin Experiment Ophthalmol. 2008;36(9):836-41. https://doi.org/10.1111/j.1442-9071.2009.01922.x.
- Casson RJ, Walker JC, Newland HS. Four-year review of open eye injuries at the Royal Adelaide Hospital: four-year review of open eye injuries. Clin Experiment Ophthalmol. 2002;30(1):15-8. https://doi.org/10.1046/j.1442-9071.2002.00484.x.
- Koo L, Kapadia MK, Singh RP, Sheridan R, Hatton MP. gender differences in etiology and outcome of open globe injuries. J Trauma Inj Infect Crit Care. 2005;59(1): 175-8. https://doi.org/10.1097/01.TA.0000173624.37438.D6.
- Blomdahl S, Norell S. Perforating eye injury in the Stockholm population. An epide- miological study. Acta Ophthalmol. 1984;62(3):378-90. https://doi.org/10.1111/j. 1755-3768.1984.tb08418.x.
- Parver LM, Dannenberg AL, Blacklow B, Fowler CJ, Brechner RJ, Tielsch JM. Charac- teristics and causes of penetrating eye injuries reported to the National eye Trauma System Registry, 1985-91. Public Health Rep Wash DC 1974. 1993;108(5):625-32.
- Colby K. Management of open globe injuries. Int Ophthalmol Clin. 1999;39(1): 59-69. https://doi.org/10.1097/00004397-199903910-00008.
- Vinger PF, Mieler WF, Oestreicher JH, Easterbrook M. Ruptured globes following ra- dial and hexagonal keratotomy surgery. Arch Ophthalmol Chic Ill 1960. 1996;114 (2):129-34. https://doi.org/10.1001/archopht.1996.01100130123001.
- Walkden A, Burkitt Wright E, Au L. Brittle cornea syndrome: current perspectives. Clin Ophthalmol. 2019;13:1511-6. https://doi.org/10.2147/OPTH.S185287.
- Treurniet S, Burger P, Ghyczy EAE, et al. Ocular characteristics and complications in patients with osteogenesis imperfecta: a systematic review. Acta Ophthalmol. 2022;100(1). https://doi.org/10.1111/aos.14882.
- Kawashima M, Kawakita T, Shimmura S, Tsubota K, Shimazaki J. Characteristics of traumatic globe rupture after keratoplasty. Ophthalmology. 2009;116(11): 2072-6. https://doi.org/10.1016/j.ophtha.2009.04.047.
- Peacock LW, Slade SG, Martiz J, Chuang A, Yee RW. Ocular integrity after refractive procedures. Ophthalmology. 1997;104(7):1079-83. https://doi.org/10.1016/ S0161-6420(97)30182-1.
- Lesniak SP, Bauza A, Son JH, et al. Twelve-year review of pediatric traumatic open globe injuries in an urban U.S. population. J Pediatr Ophthalmol Strabismus. 2012;49(2):73-9. https://doi.org/10.3928/01913913-20110712-02.
- Rostomian K, Thach AB, Isfahani A, Pakkar A, Pakkar R, Borchert M. Open globe in- juries in children. J AAPOS Off Publ Am Assoc Pediatr Ophthalmol Strabismus. 1998;2(4):234-8. https://doi.org/10.1016/s1091-8531(98)90058-1.
- Teixeira SM, Bastos RR, Falcao MS, Falcao-Reis FM, Rocha-Sousa AA. Open-globe in- juries at an emergency department in Porto, Portugal: clinical features and prog- nostic factors. Eur J Ophthalmol. 2014;24(6):932-9. https://doi.org/10.5301/ejo. 5000471.
- Kanoff JM, Turalba AV, Andreoli MT, Andreoli CM. Characteristics and outcomes of work-related open globe injuries. Am J Ophthalmol. 2010;150(2):265-269.e2. https://doi.org/10.1016/j.ajo.2010.02.015.
- Rufer F, Peters A, Klettner A, Treumer F, Roider J. Influence of alcohol consumption on incidence and severity of open-globe eye injuries in adults. Graefes Arch Clin Exp Ophthalmol Albrecht Von Graefes Arch Klin Exp Ophthalmol. 2011;249(12): 1765-70. https://doi.org/10.1007/s00417-010-1533-4.
- Mir TA, Canner JK, Zafar S, Srikumaran D, Friedman DS, Woreta FA. Characteristics of open globe injuries in the United States from 2006 to 2014. JAMA Ophthalmol. 2020;138(3):268. https://doi.org/10.1001/jamaophthalmol.2019.5823.
- Greven CM, Engelbrecht NE, Slusher MM, Nagy SS. Intraocular foreign bodies: man- agement, prognostic factors, and visual outcomes. Ophthalmology. 2000;107(3): 608-12. https://doi.org/10.1016/s0161-6420(99)00134-7.
- Roper-Hall MJ. Review of 555 cases of intra-ocular foreign body with special refer- ence to prognosis. Br J Ophthalmol. 1954;38(2):65-99. https://doi.org/10.1136/bjo. 38.2.65.
- Williams DF, Mieler WF, Abrams GW. Intraocular foreign bodies in Young people. Retina Phila Pa. 1990;10(Suppl. 1):S45-9. https://doi.org/10.1097/00006982- 199010001-00007.
- Yu TSI, Liu H, Hui K. A case-control study of eye injuries in the workplace in Hong Kong. Ophthalmology. 2004;111(1):70-4. https://doi.org/10.1016/j.ophtha.2003. 05.018.
- Bord SP, Linden J. Trauma to the globe and orbit. Emerg Med Clin North Am. 2008; 26(1):97-123. https://doi.org/10.1016/j.emc.2007.11.006.
- Hatton MP, Thakker MM, Ray S. Orbital and adnexal trauma associated with open- globe injuries. Ophthal Plast Reconstr Surg. 2002;18(6):458-61. https://doi.org/10. 1097/00002341-200211000-00013.
- Heathcote J. The ocular adnexa. Saudi J Ophthalmol. 2021;35(3):167. https://doi. org/10.4103/SJOPT.SJOPT_43_22.
- Chronopoulos A, Ong JM, Thumann G, Schutz JS. Occult globe rupture: diagnostic and treatment challenge. Surv Ophthalmol. 2018;63(5):694-9. https://doi.org/10. 1016/j.survophthal.2018.04.001.
- Skidmore C, Saurey T, Ferre RM, Rodriguez-Brizuela R, Spaulding J, Lundgreen Mason N. A narrative review of common uses of ophthalmic ultrasound in emer- gency medicine. J Emerg Med. 2021;60(1):80-9. https://doi.org/10.1016/j. jemermed.2020.08.003.
- Iyer MN, Kranias G, Daun ME. Post-traumatic endophthalmitis involving clostrid- ium tetani and Bacillus spp. Am J Ophthalmol. 2001;132(1):116-7. https://doi. org/10.1016/s0002-9394(00)00948-x.
- Romaniuk VM. Ocular trauma and other catastrophes. Emerg Med Clin North Am. 2013;31(2):399-411. https://doi.org/10.1016/j.emc.2013.02.003.
- Lesk MR, Ammann H, Marcil G, Vinet B, Lamer L, Sebag M. The penetration of oral ciprofloxacin into the aqueous humor, vitreous, and subretinal fluid of humans. Am J Ophthalmol. 1993;115(5):623-8. https://doi.org/10.1016/s0002-9394(14)71460- 6.
- Garcia-Saenz MC, Arias-Puente A, Fresnadillo-Martinez MJ, Carrasco-Font C. Human aqueous humor levels of oral ciprofloxacin, levofloxacin, and moxifloxacin.
J Cataract Refract Surg. 2001;27(12):1969-74. https://doi.org/10.1016/s0886-3350 (01)00997-x.
- Hariprasad SM, Shah GK, Mieler WF, et al. Vitreous and aqueous penetration of orally administered moxifloxacin in humans. Arch Ophthalmol Chic Ill 1960. 2006;124(2):178-82. https://doi.org/10.1001/archopht.124.2.178.
- Ahmed Y, Schimel AM, Pathengay A, Colyer MH, Flynn HW. Endophthalmitis fol- lowing open-globe injuries. Eye. 2012;26(2):212-7. https://doi.org/10.1038/eye. 2011.313.
- Abbatemarco JR, Patell R, Buccola J, Willis MA. Acute monocular vision loss: Don’t lose sight of the differential. Rutecki GW, ed. Cleve Clin J Med. 2017;84(10): 779-87. https://doi.org/10.3949/ccjm.84a.16096.
- Prasad S, Galetta SL. Approach to the patient with acute monocular visual loss. Neurol Clin Pract. 2012;2(1):14-23. https://doi.org/10.1212/CPJ.0b013e31824cb084.
- Jun B. Diagnostic considerations in patients presenting with Transient vision loss. Mo Med. 2016;113(1):63-7.
- Melen O. Two common neuro-ophthalmic problems. Optic neuritis and transient Visual disturbances. Postgrad Med. 1985;78(8). https://doi.org/10.1080/ 00325481.1985.11699226. 137-140, 142-143, 146.
- Grzybowski A, Elikowski W, Gaca-Wysocka M. Cardiovascular risk factors in pa- tients with combined central retinal vein occlusion and cilioretinal artery occlu- sion: case report. Medicine (Baltimore). 2018;97(1):e9255. https://doi.org/10. 1097/MD.0000000000009255.
- Galloway G, Wertheim M, Broadway D. Acute glaucoma with abdominal pain. J R Soc Med. 2002;95(11):555-6. https://doi.org/10.1177/014107680209501111.
- Vortmann M, Schneider JI. Acute monocular visual loss. Emerg Med Clin North Am. 2008;26(1):73-96. https://doi.org/10.1016/j.emc.2007.11.005.
- Prum BE, Herndon LW, Moroi SE, et al. Primary angle closure preferred practice pattern((R)) guidelines. Ophthalmology. 2016;123(1):P1-P40. https://doi.org/10. 1016/j.ophtha.2015.10.049.
- Hansapinyo L, Vivattanaseth C. Clinical characteristics, Treatment outcomes and predictive factors in optic neuritis. Open Ophthalmol J. 2018;12:247-55. https:// doi.org/10.2174/1874364101812010247.
- Rudkin AK, Lee AW, Chen CS. Central retinal artery occlusion: timing and mode of presentation. Eur J Neurol. 2009;16(6):674-7. https://doi.org/10.1111/j.1468- 1331.2009.02616.x.
- Ip MS. Treatment of central retinal vein occlusion-a new look at a blast from the past. JAMA Ophthalmol. 2018;136(12):1397-8. https://doi.org/10.1001/ jamaophthalmol.2018.4997.
- Sammel AM, Fraser CL. Update on giant cell arteritis. Curr Opin Ophthalmol. 2018; 29(6):520-7. https://doi.org/10.1097/ICU.0000000000000528.
- Beshay N, Keay L, Dunn H, Kamalden TA, Hoskin AK, Watson SL. The epidemiology of open globe injuries presenting to a tertiary referral eye hospital in Australia. In- jury. 2017;48(7):1348-54. https://doi.org/10.1016/j.injury.2017.04.035.
- Mayer CS, Reznicek L, Baur ID, Khoramnia R. Open globe injuries: classifications and prognostic factors for functional outcome. Diagn Basel Switz. 2021;11(10): 1851. https://doi.org/10.3390/diagnostics11101851.
- Yuan WH, Hsu HC, Cheng HC, et al. CT of globe rupture: analysis and frequency of findings. Am J Roentgenol. 2014;202(5):1100-7. https://doi.org/10.2214/AJR.13. 11010.
- Russell SR, Olsen KR, Folk JC. Predictors of scleral rupture and the role of vitrectomy in severe blunt ocular trauma. Am J Ophthalmol. 1988;105(3):253-7. https://doi. org/10.1016/0002-9394(88)90005-0.
- Crowell EL, Koduri VA, Supsupin EP, et al. Accuracy of computed tomography imag- ing criteria in the diagnosis of adult open globe injuries by neuroradiology and ophthalmology. Jang TB, ed. Acad Emerg Med. 2017;24(9):1072-9. https://doi. org/10.1111/acem.13249.
- Kubal WS. Imaging of orbital trauma. Radiogr Rev Publ Radiol Soc N Am Inc. 2008; 28(6):1729-39. https://doi.org/10.1148/rg.286085523.
- Sung EK, Nadgir RN, Fujita A, et al. Injuries of the globe: what can the radiologist offer? Radiogr Rev Publ Radiol Soc N Am Inc. 2014;34(3):764-76. https://doi.org/ 10.1148/rg.343135120.
- Adesanya OO, Dawkins DM. Intraorbital wooden foreign body (IOFB): mimicking air on CT. Emerg Radiol. 2007;14(1):45-9. https://doi.org/10.1007/s10140-007- 0576-2.
- LeBedis CA, Sakai O. Nontraumatic orbital conditions: diagnosis with CT and MR imaging in the emergent setting. RadioGraphics. 2008;28(6):1741-53. https:// doi.org/10.1148/rg.286085515.
- Kim SY, Lee JH, Lee YJ, et al. Diagnostic value of the anterior chamber depth of a globe on CT for detecting open-globe injury. Eur Radiol. 2010;20(5):1079-84. https://doi.org/10.1007/s00330-009-1653-6.
- Patel SN, Langer PD, Zarbin MA, Bhagat N. Diagnostic value of clinical examination and radiographic imaging in identification of intraocular foreign bodies in open globe injury. Eur J Ophthalmol. 2012;22(2):259-68. https://doi.org/10.5301/EJO. 2011.8347.
- Go JL, Vu VN, Lee KJ, Becker TS. Orbital trauma. Neuroimaging Clin N Am. 2002;12 (2):311-24. https://doi.org/10.1016/S1052-5149(02)00012-6.
- Joseph DP, Pieramici DJ, Beauchamp NJ. Computed tomography in the diagnosis and prognosis of open-globe injuries. Ophthalmology. 2000;107(10):1899-906. https://doi.org/10.1016/s0161-6420(00)00335-3.
- Arey ML, Mootha VV, Whittemore AR, Chason DP, Blomquist PH. Computed tomog- raphy in the diagnosis of occult open-globe injuries. Ophthalmology. 2007;114(8): 1448-52. https://doi.org/10.1016/j.ophtha.2006.10.051.
- Ojaghihaghighi S, Lombardi KM, Davis S, Vahdati SS, Sorkhabi R, Pourmand A. Diag- nosis of traumatic eye injuries with point-of-care Ocular ultrasonography in the emergency department. Ann Emerg Med. 2019;74(3):365-71. https://doi.org/10. 1016/j.annemergmed.2019.02.001.
- Blaivas M, Theodoro D, Sierzenski PR. A study of bedside ocular ultrasonography in the emergency department. Acad Emerg Med Off J Soc Acad Emerg Med. 2002;9
(8):791-9. https://doi.org/10.1111/j.1553-2712.2002.tb02166.x.
- Pfeiffer P, Marco C. 348: UltraSonographic detection of intraocular foreign bodies. Ann Emerg Med. 2008;52(4):S148.
- Blaivas M. Bedside emergency department ultrasonography in the evaluation of oc- ular pathology. Acad Emerg Med. 2000;7(8):947-50. https://doi.org/10.1111/j. 1553-2712.2000.tb02080.x.
- Blanch RJ, Bishop J, Javidi H, Murray PI. Effect of time to Primary repair on final vi- sual outcome after open globe injury. Br J Ophthalmol. 2019;103(10):1491-4. https://doi.org/10.1136/bjophthalmol-2017-311559.
- Rahman I, Maino A, Devadason D, Leatherbarrow B. Open globe injuries: factors predictive of poor outcome. Eye (Lond). 2006;20(12):1336-41. https://doi.org/ 10.1038/sj.eye.6702099.
- Man CYW, Steel D. Visual outcome after open globe injury: a comparison of two prognostic models-the ocular trauma score and the classification and regression tree. Eye. 2010;24(1):84-9. https://doi.org/10.1038/eye.2009.16.
- Huang JM, Pansick AD, Blomquist PH. Use of intravenous vancomycin and cefepime in preventing endophthalmitis after open globe injury. J Ocul Pharmacol Ther Off J Assoc Ocul Pharmacol Ther. 2016;32(7):437-41. https://doi.org/10.1089/jop.2016. 0051.
- Gao H, Pennesi ME, Shah K, et al. Intravitreal voriconazole: an electroretinographic and histopathologic study. Arch Ophthalmol Chic Ill 1960. 2004;122(11):1687-92. https://doi.org/10.1001/archopht.122.11.1687.
- Smiddy WE. Treatment outcomes of endogenous fungal endophthalmitis. Curr Opin Ophthalmol. 1998;9(3):66-70. https://doi.org/10.1097/00055735- 199806000-00012.
- Samiy N, D’Amico DJ. Endogenous fungal endophthalmitis. Int Ophthalmol Clin. 1996;36(3):147-62. https://doi.org/10.1097/00004397-199603630-00014.
- Borne MJ. Ocular fluconazole treatment of Candida parapsilosis endophthalmitis after failed intravitreal amphotericin B. Arch Ophthalmol. 1993;111(10):1326. https://doi.org/10.1001/archopht.1993.01090100032019.
- Cebulla CM, Flynn HW. Endophthalmitis after open globe injuries. Am J Ophthalmol. 2009;147(4):567-8. https://doi.org/10.1016/j.ajo.2008.12.016.
- Aguilar HE, Meredith TA, Shaarawy A, Kincaid M, Dick J. Vitreous cavity penetration of ceftazidime after intravenous administration. Retina Phila Pa. 1995;15(2):154-9. https://doi.org/10.1097/00006982-199515020-00012.
- Cruvinel Isaac DL, Ghanem VC, Nascimento MA, Torigoe M, Kara-Jose N. Prognostic factors in open globe injuries. Ophthalmol J Int Ophtalmol Int J Ophthalmol Z Augenheilkd. 2003;217(6):431-5. https://doi.org/10.1159/000073075.
- Pieramici DJ, MacCumber MW, Humayun MU, Marsh MJ, de Juan E, Open-globe in- jury. Update on types of injuries and visual results. Ophthalmology. 1996;103(11): 1798-803. https://doi.org/10.1016/s0161-6420(96)30424-7.
- Lee CH, Lee L, Kao LY, Lin KK, Yang ML. prognostic indicators of open globe injuries in children. Am J Emerg Med. 2009;27(5):530-5. https://doi.org/10.1016/j.ajem. 2008.04.004.
- Scott R. The ocular trauma score. Community Eye Health. 2015;28(91):44-5.
- Bhagat N, Li X, Zarbin M. Pediatric open globe injury: a review of the literature. J Emerg Trauma Shock. 2015;8(4):216. https://doi.org/10.4103/0974-2700.166663.