
Swyer-James-Macleod syndrome: a rare finding and important differential in the ED setting
Abstract
Swyer-James-Macleod syndrome is a rare pulmonary disorder. It is characterized as a constrictive bronchiolitis resulting from loss of pulmonary vascularity secondary to a previous upper respiratory infection.
We present the case of a 5-year-old boy who presented to the emer- gency department (ED) for acute asthma exacerbation. radiographic imaging confirmed the diagnosis of Swyer-James-Macleod syndrome. The patient was admitted to the pediatric floor and treated with symptomatic management and discharged home after complete resolution of symptoms.
Swyer-James syndrome is a rare disease that should be considered in individuals with recurrent pulmonary infections and hyperactive airway disease. Radiographic or Computed tomography imaging is required in such patients for diagnosis.
Swyer-James-Macleod syndrome is an extremely rare radiographic finding characterized by unilateral pulmonary hyperlucency. This diag- nostic finding is a long-term sequela of bronchiolitis obliterans. Presen- tation of this syndrome is characterized by dyspnea, hemoptysis, reactive upper airway disease, and recurrent pulmonary infections. The etiology of this syndrome is diverse, as are its Long-term effects. This rare disease causes a unique diagnostic challenge in the ED where the presenting sign is often an acute asthma exacerbation as witnessed in our patient. In the setting of both pediatric and adult patients, Swyer- James syndrome should be considered in patients with acute asthma exacerbation and a positive history of upper Respiratory infections.
A 5-year-old known asthmatic boy presented to the emergency de- partment (ED) with chief complaints of wheezing and Chest tightness of 1-day duration. Before presentation, the patient reported intermittent asthma for 2 weeks requiring daily use of albuterol. His symptoms worsened the day before presentation, when he began to cough and experience posttussive vomiting, chest tightness, and a tactile fever. The patient never became cyanotic or ashen. His symptoms did not improve after multiple albuterol treatments at home, after which he was brought to the ED. Medical history was positive for eczema and asthma. The patient reported allergies to egg, wheat, seafood, and animal dander. Family history was positive for asthma in both parents. There was no history of travel or sick contacts. Immunizations were up to date.
At the ED, his temperature was 98.2?F; pulse, 148 beats per minute; respiratory rate, 18 breaths per minute; blood pressure, 112/79, with SaO2 of 93% on room air. Physical examination revealed signs of moder- ate respiratory distress. nasal flaring with supraclavicular, subcostal, and intercostal retractions were noted. Auscultation of the lungs revealed poor air entry with bilateral expiratory wheezing. The rest of the examination was unremarkable.
Complete blood count and comprehensive metabolic panel were normal. A chest x ray showed decreased right lung volume with right perihilar Ground glass opacities, areas of linear scarring, and atelectasis see figure 1. These radiographic findings were consistent with a prior postinfectious bronchiolitis. Comparison to a previous chest film (taken 3 months prior) showed the same findings see figure 2.A diagno- sis of Swyer-James-MacLeod syndrome was made.
The patient was admitted and received systemic steroids and bronchodilator therapy. He was discharged in stable condition and with follow-up care scheduled with the pulmonologist.
Swyer-James-Macleod syndrome was first described in 1953 by Swyer and James and then subsequently in 1954 by Macleod [1]. Swyer-James-Macleod syndrome is a very rare lung condition that exhibits unilateral hemithorax hyperlucency that results from a postinfectious bronchiolitis, often bronchiolitis obliterans [2]. In a review of 17 450 lung radiographs performed by Yekeler, unilateral hyperluceny was found in only 0.01% of patients [3]. The diagnostic criteria for this syndrome require 1 of the following 3: unilateral loss of lung volume with hyperlucency as demonstrated by chest x-ray, uni- lateral reduction in vascularity on computed tomographic scan of the chest, or unilateral loss of perfusion on technetium Tc 99m lung scan. Unilateral hemithorax hyperlucency may result from poor patient posi- tioning; in the absence of such error, this is sufficient for diagnosis. Dif- ferential diagnosis for this finding include, but are not limited to, mastectomy, pneumothorax, pleural effusion, mediastinal fibrosis, gas- trointestinal herniation, bronchial compression, obliterative bronchioli- tis, pulmonary emphysema, and pulmonary embolism. Swyer-James- Macleod syndrome is late sequela of infectious bronchiolitis that occurs during childhood. causative organisms involved include Mycoplasma pneumonia, influenza A, mycobacteria, Bordetella pertussis, adenovirus, paramyxovirus, and measles [4]. The infectious agent results in an in- flammatory response, which causes obliteration of peripheral airways in the infected lung. This inflammation results in obliteration of the vas- cularity of the lung and impeded lung development. Long-term effects on the lung are destruction of the alveoli and dilation of the pulmonary parenchyma [3]. Early infection results in the destruction and subse- quent fibrosis of the bronchioles destructing the development of the al- veolar bud [5]. This underdevelopment of the lung causes poor air intake and results in the classic findings seen on imaging of affected lungs. Adult manifestations of this infectious process include bronchiec- tasis, chest pain, wheezing, recurrent bronchitis, hemoptysis, recurrent pneumonia, and bronchial hyperresponsiveness [3, 6]. Given that the age of initial infection usually occurs early on in life, diagnosis is not typ- ically caught until later symptoms of the syndrome cause concern, prompting imaging. Ventilation perfusion scans of patients who have Swyer-James-Macleod syndrome shows decrease exchange of gas in
0735-6757/(C) 2015 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).

Fig. 1. Chest x-ray demonstrating hyperlucency confirming Swyer-James-Macleod syndrome.
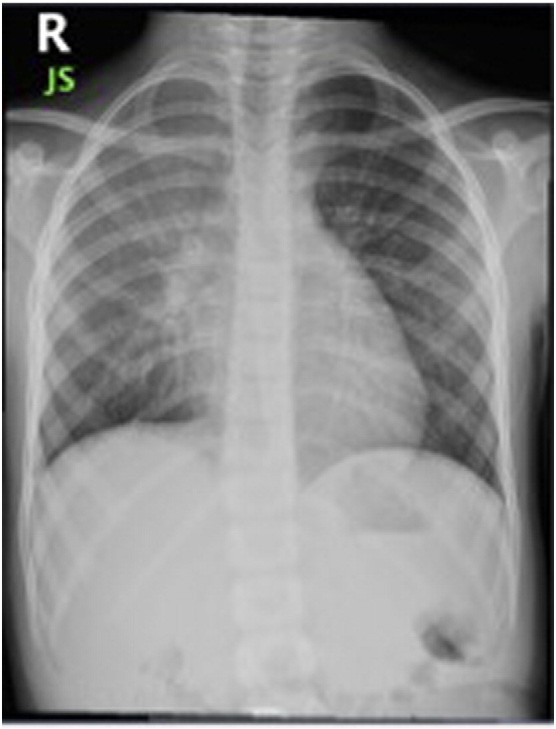
Fig. 2. X-ray taken 3 months before visit demonstrating unilateral hyperlucency.
the ventilatory phase [7]. Understanding this pathology is especially im- portant in the ED setting where imaging may be confused for pneumothorax resulting in unnecessary chest tube placement [8]. This pathology should also be considered in patients who have been di- agnosed as asthmatics who appear to be nonresponsive to conventional
therapy. Reports in the literature have shown misdiagnosis of asthma in patients who later were diagnosed with Swyer-James-Macleod syn- drome when the appropriate imaging was performed [9]. The most concerning long-term effects of this syndrome is recurrent lung infections. In patients in whom this is seen, symptomatic management is the treatment of choice in conjunction with prompt and effective antibiotic therapy. Surgery is an option in patients who experience unrelenting infections or when an entire lung is affected. In most patients with Swyer-James-Macleod syndrome, treatment is managed by chest physiotherapy, low-dose inhaled corticosteroids, and Inhaled bronchodilators. This differential remains important in patients presenting to the ED with chief compliant of shortness of breath. A hyperlucent lung field is an alarming radiographic finding. Before drastic measures are initiated, radiographic images should be assed to guide both short- and Long-term treatment options.
Benjamin Chaucer, BS Marie Chevenon, BSc, MSc
St Georges University School of Medicine, St Georges, Grenada
Corresponding author
E-mail address: [email protected]
Cloty Toro, MD
Richmond University Medical Center (RUMC), Staten Island, NY
Teresa Lemma, MD
Pediatric Medicine Department, RUMC, Staten Island, NY
Melissa Grageda, MD
Department of Pediatric Critical Care Medicine, RUMC, Staten Island, NY
http://dx.doi.org/10.1016/j.ajem.2015.12.045
References
- AhatCimen D, et al. Delayed diagnosis in a patient with bronchiectasis: Swyer-James- Macleod syndrome. Respir Case Rep 2013;2(1):39-43 [Web].
- Jones, Jeremy. Swyer-James Syndrome | Radiology Reference Article | Radiopaedia. Org. Radiopaedia.org. N.p., 2015. Web. 20 Nov. 2015.
- Yekeler E. A rare case of Swyer-James Macleod syndrome and a new clinical presentation, acquired lobar emphysema. Ann Thorac Surg 2012;93(5):e123-5 [Web].
- Damle NA, Mishra R, KaurWadhwa J. Classical imaging triad in a very young child with Swyer-James syndrome. Nucl Med Mol Imaging 2012;46(2):115-8 [Web].
- Lucaya J, et al. Spectrum of manifestations of Swyer-James-Macleod syndrome.
J Comput Assist Tomogr 1998;22(4):592-7 [Web].
Macleod WM. Abnormal transradiancy of one lung. Thorax 1954;9(2):147-53 [Web].
- Chuang T-L, Wang Y-F, Lai C-L. Ventilation-perfusion SPECT/CT. Diagnosing Swyer-James (Macleod) syndrome, 22.4. Tzu Chi Medical Journal; 2010. p. 213-8 [Web].
- Sulaiman A, et al. Swyer-James-Macleod syndrome; repeated chest drainages in a
patient misdiagnosed with pneumothorax. Interact Cardiovasc Thorac Surg 2009; 8(4):482-4 [Web].
Walia M, Goyal V, Jain P. Swyer-James-Macleod syndrome in a 10-year-old boy misdiagnosed as asthma. Indian J Pediatr 2010;77(6):709 [Web].